Fracture of Neck of Femur (NOF) – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Fracture of Neck of Femur (NOF)
Characteristics of Fracture of NOF:
1) Increasing incidence with age is thought to be secondary to bone density loss.
2) Commoner in elderly females; below the age of 60, men are affected more frequently (usually extra capsular fractures).
3) Seen more commonly in patients taking a variety of medications, such as corticosteroids, thyroxine, phenytoin and frusemide.
4) Most related to only minor trauma.
Classification of Fracture of Neck of Femur (NOF):
A) On the basis of capsule:
1) Intracapsular fracture(blood supply to femoral head damaged):
a) Subcapital,
b) Transcervical
2) Extra-Capsular (blood supply intact):
a) Trochanteric
b) Sub trochanteric
B) Based on degree on displacement of fracture (Garden classification):
Intracapsular fracture of neck of femur classified according to Garden at Grades I-IV.
Grades-I (Incomplete): Inferior cortex is not completely broken.
Grade-II(Complete): Inferior cortex also clearly broken. Trabecular pattern interrupted but not angulated.
Grade-III(Slightly displaced): Angulated trabecular pattern.
Grade-IV( Fully displaced): Severest grade. Often no bony continuity.
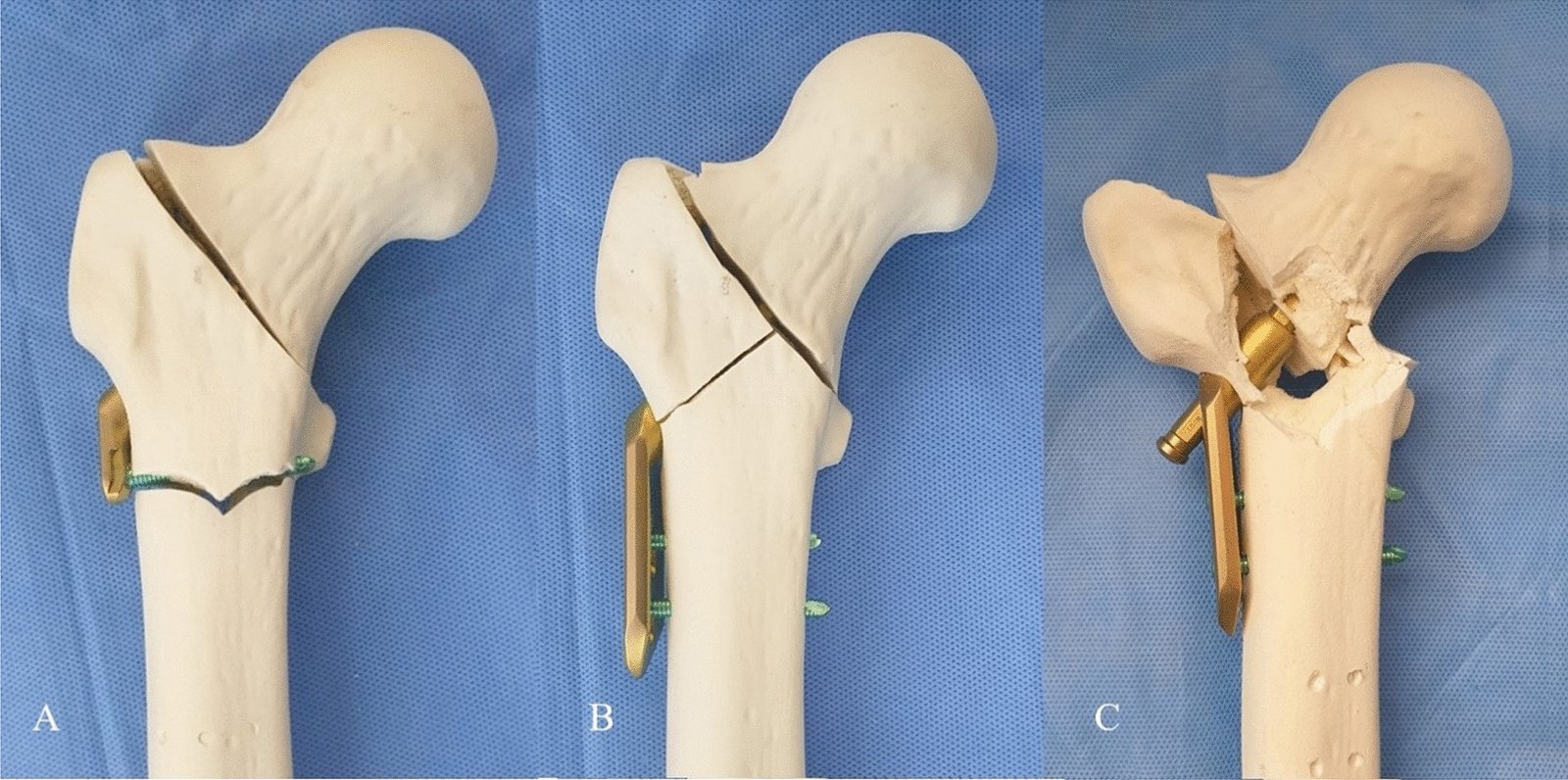
c ) Left below, Grade II intracapsular fracture, d) Grade III intracapsular fracture, e) grade iv Intracapsular fracture.
Clinical features of Fracture of Neck of Femur (NOF):
A) Patients profile:
- Age-5th-7th decade
- Sex-Mostly post menopausal women.
B) Clinical features:
1) History of trauma (Fall on flexed & rotated hip RTA, and fall from height)
2) Pain in the affected hip – increase on movement. 10
3) Unable to walk.
4) Movement of hip are restricted and painful.
5) Signs:
a) Tenderness over the hip joint line.
b) Shortening of the limb.
c) External rotational deformity
d) Active straight leg raising is difficult.
e) Patients complaints of groin pain due to impacted fracture neck of femur.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-657-658]
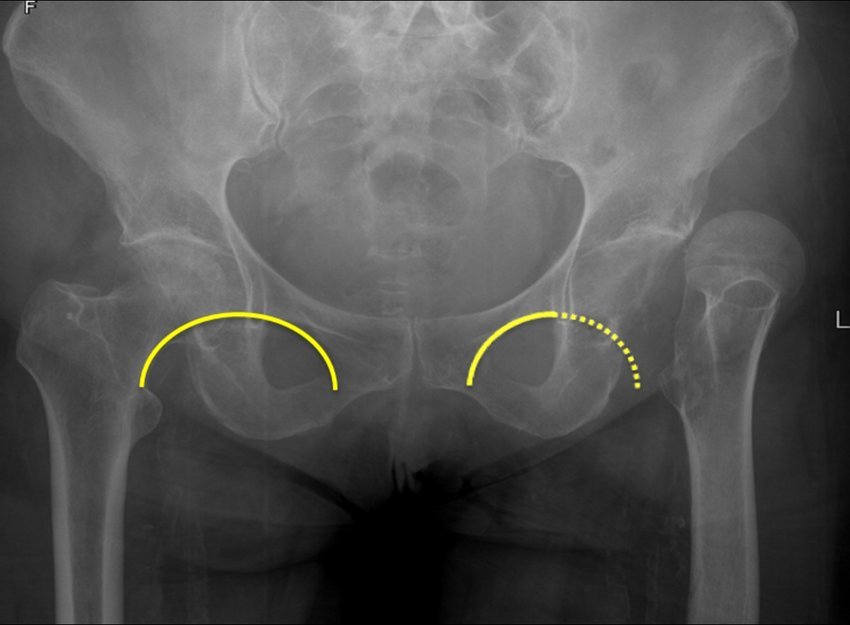
Radiological features: AP views
1) Break in the Shenton’s lines.
2) Prominent lesser trochanter.
3) Look for asymmetry. Compare Shenton’s lines on the AP view. On the lateral view check for angulation of the head in respect to the neck.
4) If suspicious, but no fracture is seen, a bone scan at 48 hours or delayed repeat film can be of benefit.
Treatment of femoral fracture: Treatment depends upon age and nature of injury –
A) Undisplaced fracture: Internal fixation by: Dynamic hip screw (Adults) Knewles pin (Children).
B) Displaced fracture:
✓ <20 Years – Closed reduction and internal fixation with Knewles pin.
✓ <40 Years = Closed reduction and internal fixation with hip screw.
✓ >65 Years= Excision of femoral head and replacement by a prosthesis.

C) Rest for 12 weeks.
D) Exercise: First 3 months non weight bearing.
[Ref-Dr. Jahir, “Surgery I” Paper” 4th Edition,Page-556]
Modern treatment of Femoral neck fracture:
1) Open reduction with internal fixation (ORIF).
2) Hemiarthroplasty.
3) Total hip replacement
[Ref-Dr. Jahir, “Surgery I” Paper” 4th Edition, Page-556]
Complication of fracture neck femur:
A) Local complication: At the site of fracture.
1) Avascular necrosis of head of femur.
2) Non union,mal-union.
3) Osteoarthritis at neck of femur.
4) Limb shortening.
B) General complication: Prolonged bed rest causing.
1) Deep vein thrombosis (DVT)
2) Pulnonary embolisms.
3) Hypostatic pneumonia.
4) Progressive bed sores.
5) Nephrolithiasis.
6) Decalcification.
[Ref-Dr. Jahir, “Surgery I” Paper” 4th Edition, Page-556]
Clinical features of subtrochanteric femur fracture:
1) Pain.
2) Swelling.
3) Shortening.
4) Complete external rotation deformity.
5) Other usual features of fracture.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-227]
Treatment of subtrochanteric femur fracture:
A) Conservative: Methods are advocated if the patient is young. In severely comminuted fractures, modified cast brace with pelvic band is used.
B) Surgery: This is the preferred method of treatment in adults and ORIF is chosen for those fractures, which can be made stable by closed or open reduction.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-227]
Complications of subtrochanteric femur fracture:
1) Mal-union: This is a possibility with conservative treatment.
2) Shortening.
3) Nonunion due to soft tissue interposition and is relatively rare.
4) Secondary osteoarthritis of the hip.
5) Contralateral hip and knee pain due to limp and altered weight bearing mechanism.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-229]
Fracture shaft femur:
A. In adult:
1) RTA commonest cause.
2) Industrial accidents.
3) Fall from height.
4) Gun shot injuries.
B. In children:
1) Fall.
2) Birth injuries.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-229]
clinical features of fracture shaft femur:
A) Symptoms:
1. Pain- Severe pain on movement.
2. Swelling: Gross swelling of the thigh within a very short time.
3. Deformity: Sometimes deformity is obvious. Limb is externally rotated.
4. Loss of functions.
5. Abnormal mobility.
6. Bony crepitation.
7. Shortening.
B) Signs:
1) On examination: Dehydration.
2) Inspection: Limb is externally rotated, short and swollen.A rapidly expanding thigh suggests a large/ongoing haemorrhage.
3) Palpation:
a. Local temperature is raised.
b. On deep palpation:
c.Tenderness.
d. Abnormal mobility at the fracture site.
e. Bony crepitation may be felt.
(Ref-Dr. M.A.H.M. Jafar’s “Fracture and Dislocations” 2nd edition page-218)
Management of fracture shaft femur :
B) Displaced fracture:
1) Supportive treatment:
a) Treatment of shock.
b) Analgesics.
c) Intravenous fluid and antibiotics.
d) Skeletal traction.
2) Specific treatment: Open reduction and internal fixation with intramedullary nail.
3) <18 months Gallows traction.
4) Older children: Thomas splint and skin traction.
C) Undisplaced fracture:
1) Adult: Skeletal traction for 4-6 weeks followed by hip spica & Immobilization by long leg cast (LLC).
2) Children: Surface traction followed by hip spica.
Complications of fracture shaft femur:
A) Immediate complications: These are life threatening and the common ones )e
1) Shock.
2) Fat embolism.
3) Neurovascular injury to the femoral artery.
4) Sciatic nerve.
B) Delayed complications: These are more common and include:
1) Refracture.
2) Complications of fixation devices.
3) Nerve injury.
4) Mai union.
5) Nonunion.
6) Joint stiffness.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-236]
Nails in common usage for fixing fracture shaft femur :
1) Standard IM nails (Kuntscher’s nail): The ideal indication for this nail is the fracture shaft femur in at the level of isthmus adult
2) Interlocking nails (Gross-kempf nail): These extend the indications of standard IM nail and can be used in the following situations where IM nail is less successful.
3) Flexible medullary nails like Ender’s nail, which is usually passed from below upwards through the distal femur.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-234]
The fracture of the distal femur fracture:
1) Supracondylar fracture of femur.
2) Intercondylar fracture of femur.
3) Unicondyl ar fracture of femur.
4) Comminuted fracture of femur. (Bicondylar).
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-236]
Neer’s classification for supracondylar fractures:
1) Undisplaced fracture.
2) Displaced fracture:
a) Medial displacement.
b) Lateral displacement.
3) Comminuted fracture
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-237]
Clinical features of supracondylar fracture of femur :
1) Pain and swelling.
2) Loss of function.
3) Ecchymosis.
4) Localized tenderness.
5) Movement is too painful.
6) Hemarthrosis is commonly seen, especially with fractures extending into the joint.
7) Flexion deformity caused by the pull of gastrocenemius.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-237]
Radiological features of supracondylar fracture of femur:
Treatment of supracondylar fracture of femur:
A) Non-operative management:
1) If the fracture is only slightly displaced and extra-articular, or if it reduces easily with the knee in flexion, it can be treated quite satisfactorily by traction through the proximal tibia,
2) The limb is cradled on a Thomas’ splint with a knee flexion piece and movements are encouraged.
3) If the distal fragment is displaced by gastrocnemius pull, a second pin above the knee, and vertical traction, will correct this.
4) At 4-6 weeks, when the fracture is beginning to unite, traction can be replaced by a cast-brace
5) and the patient allowed up and partially weight bearing with crutches. Non-operative treatment should be considered as an option if the patient is young or the facilities and skill to treat by internal fixation are absent.
6) Elderly patients tend not do as well with the 6 weeks of enforced recumbency.
B) Surgical management :
Operative treatment with internal fixation can enable accurate fracture reduction, especially of the joint surface, and early movement.
a) Intramedullary fixation.
b) Blade plate fixation.
c) Dynamic condylar screw.
d) Condylar locking screw.
e) Double plate fixation.
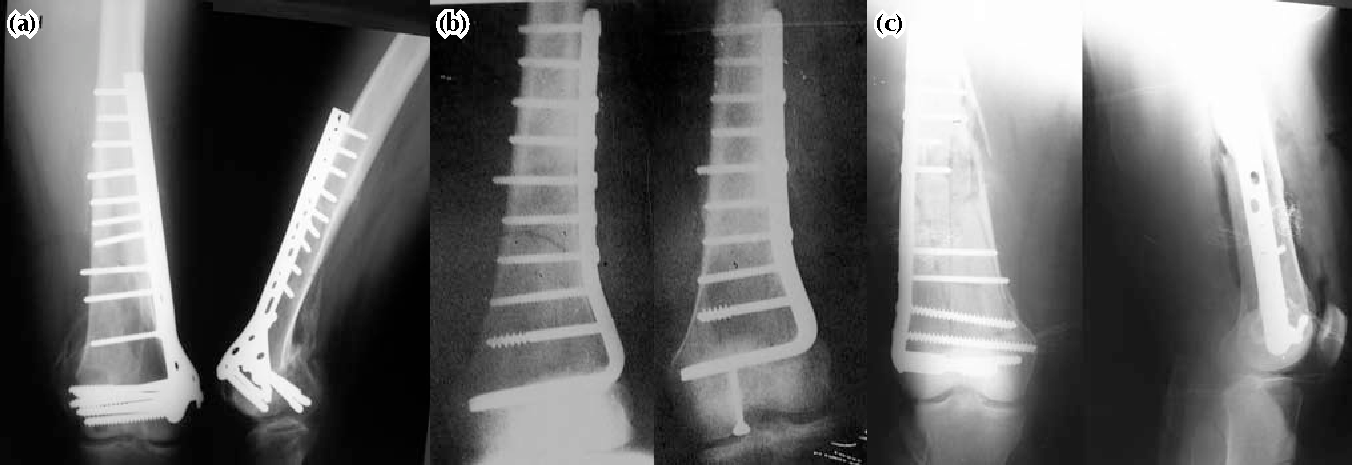
(Ref-Apley’s “System of Orthopaedics and Fractures” 9th edition page-870+ John Ebnezar’s “textbook of Orthopedics” 4th edition page-239)
Complications of supracondylar fracture of femur:
1) Delayed union.
2) Mai union.
3) Nonunion.
4) Injury to the popliteal vessels.
5) Injury to the common personeal nerves.
6) Knee stiffness.
7) Deep vein thrombosis.
8) Infection.
9) Implant failure.
[Ref-John Ebnezar’s “textbook of Orthopedics” 4th edition page-239]