Hip Dislocation – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Hip Dislocation
Anatomy of the hip joint:
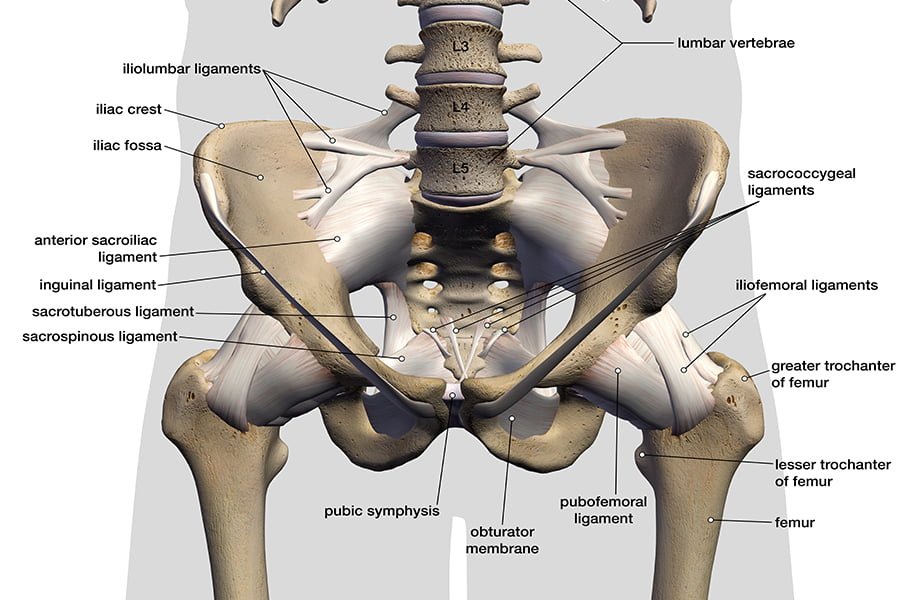
- Ball and socket type of synovial joint.
- Movements: Flexion, extension, abduction, adduction, circumduction, medial and lateral rotation.
- Head of the femur articulates with cup shaped fossa of acetabulum.
- Articular surface of the acetabulum forms an incomplete ring termed as lunate ring.
- Capsule surrounded by muscles on all sides
Types of hip dislocation: On the basis of site of dislocations,
1) Posterior hip dislocation(95%).
2) Anterior hip dislocation(5%).
3) Central hip dislocation (rare).
Clinical features of the hip joint dislocation:
A) History: History of trauma, (RTA, fall from height, air crush).
B) Symptoms:
1. Pain on the injured hip joint.
2. Deformity of the limb.
3. Restricted movement of the hip.
C) Signs:
1) Deformity of the limb: Shortening of limb & limb flexed,adducted and internl rotated,
2) A hard mass due to displaced head in the gluteal region sometimes may be seen and felt.
3) Restricted movement of the hip.
4) Impairment of function of sciatic nerve.
5) General examination: To see bony injuries in patella, head of femur, Supracondular fracture, chest data and pelvis fracture etc.
[Ref-Dr. Jahir, Surgery, paper-1, 4th edition. page-539]
Treatment of hip dislocation:
1) Complete bed rest.
2) Immobilize the patients and keep comfortable positions.
3) Immediate closed reduction under G/A.
4) External traction postoperatively for 6 weeks and start active movement as soon as pain subsides.
5) After 4 weeks non weight bearing walking. 6) After 12 weeks weight bearing walking.
[Ref-Dr.Jahir, Surgery, paper-1, 4th edition. page-539]
Complication of the hip dislocation:
A) Early complication:
1) Sciatic nerve injury.
2) Vascular injury.
3) Associate fractured and femoral shaft stiffness.
B) Late complication:
1) Avascular necrosis.
2) Myositis ossification.
3) Osteoarthritis
4) Unreduced dislocation.
5) Delayed union.
[Ref-Apleys, System of Orthpedics and fracture, 9th edition,page-845]
Hip dislocation rare, because:
- The acetabular cavity is deep.
- Joint is surrounded by strong muscles and ligaments which eventually supports the joint.
Shoulder dislocation spontaneously occurs due to,
1) Shallowness of the glenoid socket.
2) Extraordinary range of movement.
3) Ligamentous laxity.
4) GLenoid dysplasia
5) Sheer vulnerability of the joint during stressful activity of the upper limb.
Nursing management of hip dislocation patients:
A) Alleviating pain:
1) Traction by continuous pull to reduce pain.
2) Provide pain and muscle relaxant medications.
3) Encourage the patients to use relaxation techniques.
B) Increase mobility:
1) Patients maintain traction with correct body alignment.
2) Encourages the patients to use trapezeus muscle and unaffected limb to change positions in bed.
3) Monitor correct weight application required for tractions.
4) Encourage the patients to do gluteal and quadriceps exercise, ankle pump, flexion, extension of legs and active ROM of the unaffected hip.
5) To avoid extreme abduction and external rotation.
6) As patients has obtained painless range of motion in affected hip, weight bearing as resumed.
C) Improving knowledge about treatment methods:
1) Knowledge of exercise.
2) Intake regular medications.
3) Clean the bed linen, cloths and operative area.
4) Intake of nutritious food beneficiaries for bone healing.
[Ref-Lippincott, Adult Orthopedic Nursing, I edition, Page-274,275]
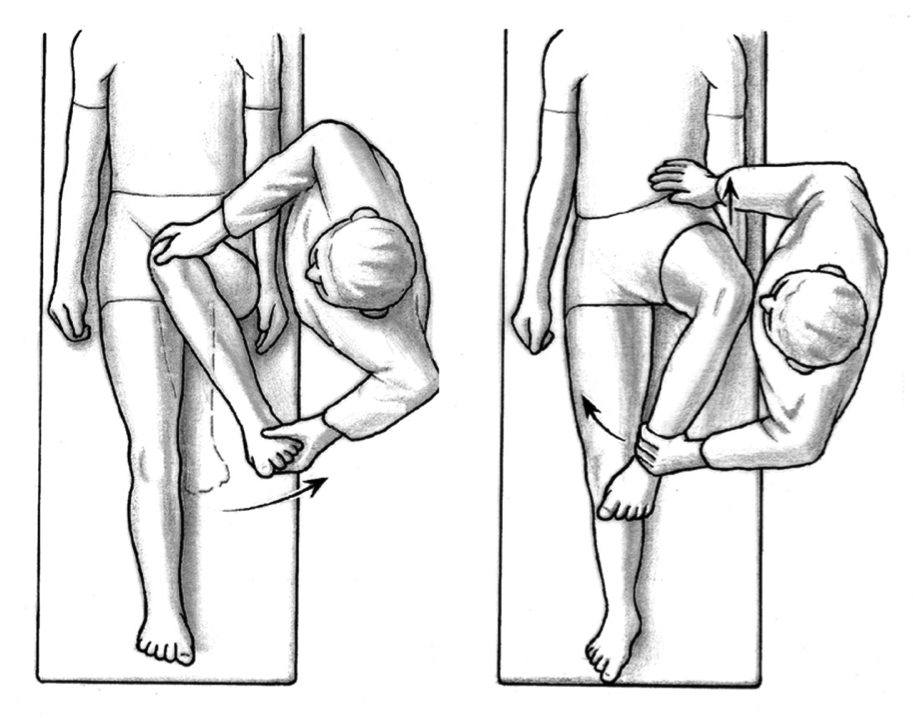
Reduction in posterior hip dislocation patients:
The common treatment for posterior dislocation is immediate closed reduction within 24 hours. Following injury:
1) Give intravenous analgesics, muscle relaxants, general anesthesia.
2) Patients is positioned in supine positions.
3) Patients pelvis is stabilizes by pressure on both anterior spine by an assistant.
4) The physician then applies traction in the direct line of the deformity followed by gentle flexion of the hip to 90 degrees.
5) The hip is then rotated internally and externally with continued longitudinal traction. Until reduction is accomplished,
6) Most reduction can be accomplished without open surgery.
[Ref-Lippincott,Adult Orthopedic Nursing, I” edition, Page-272]