Giant Cell Tumor -An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Giant Cell Tumor
Definition of osteoclastoma:
Osteoclastoma (Giant cell tumor) is an aggressive but benign tumor which appears in mature bone, most commonly in the distal femur, proximal humerus and distal radius.
[Ref- Apley’s “System of orthopedics and fractures”, 9h edition, P-202]
Or
Cell tumor is an osteolytic tumor arising from the epiphysis and is common in young adults.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, 4″ edition, P-631]
Sites of giant cell tumors:
1. Distal femur: 28%
2. Proximal tibia: 8%
3. Proximalfemur: 5%
4. Proximal humerus: 3%
5. Distal radius, three: 3%
6. Distal humerus, four: 4%
7. Sacrum: 3%
8. Ilium: 2%
9. Talus: 1%
10. Metacarpal joint: 1%
[Ref-W.Jehn, Journal of bone and joint surgery, 2004]
Osteoclastoma is called giant cell tumor:
Presence of abundant tumor giant cell in case of osteoclastoma.Each cells contains 50-150 nuclei.
Clinical features of osteoclastoma:
1) Age-Common in young adult between 20-40 years. 2) Site- Knee, Distal radius, proximal humerus.
3) Dull aching pain at the site of tumor.
4) Gradually increasing local swellings.
5) Pathological fracture.
6) Tender on firm palpation.
[Ref-Adams/11 edition, P-/86,87]
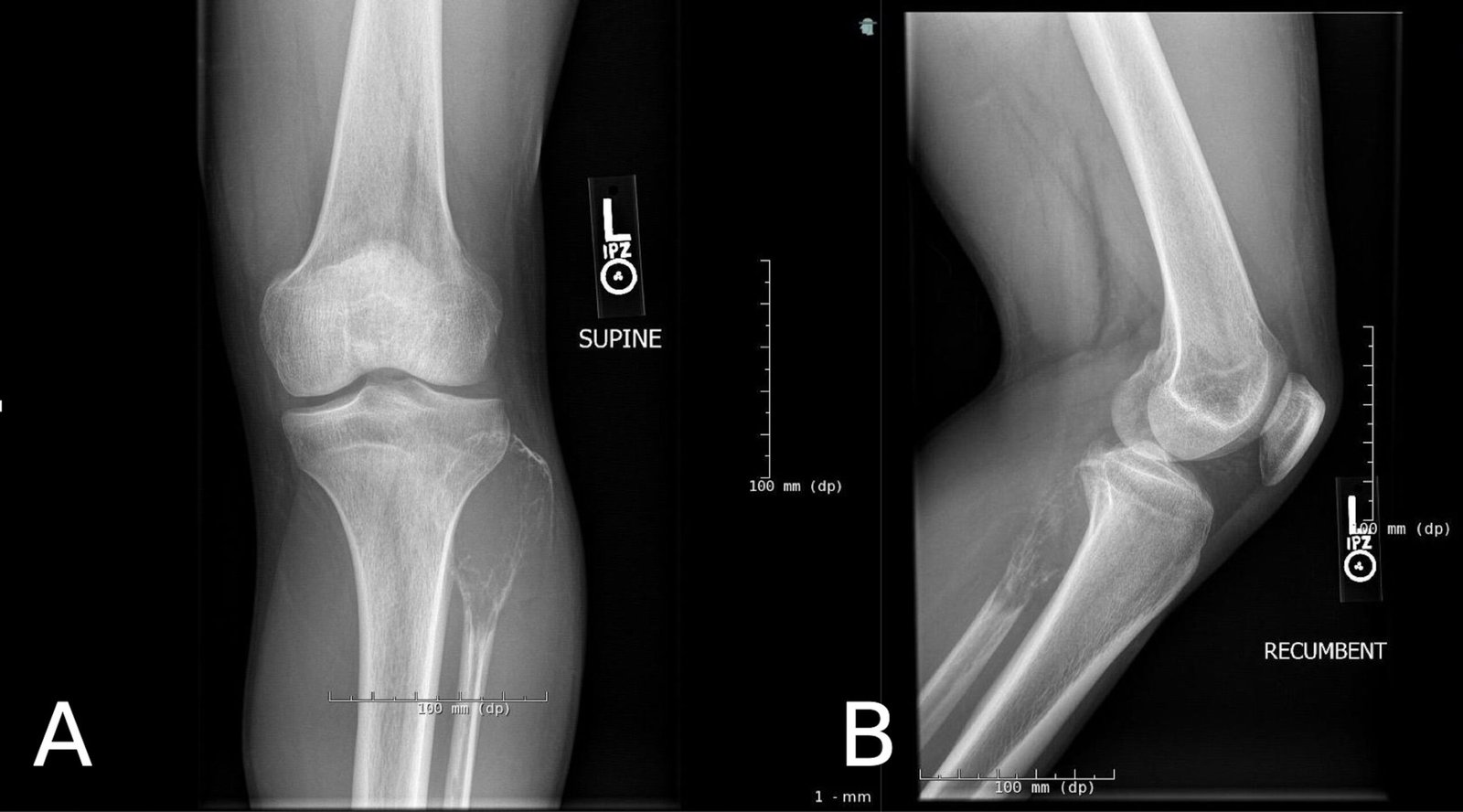
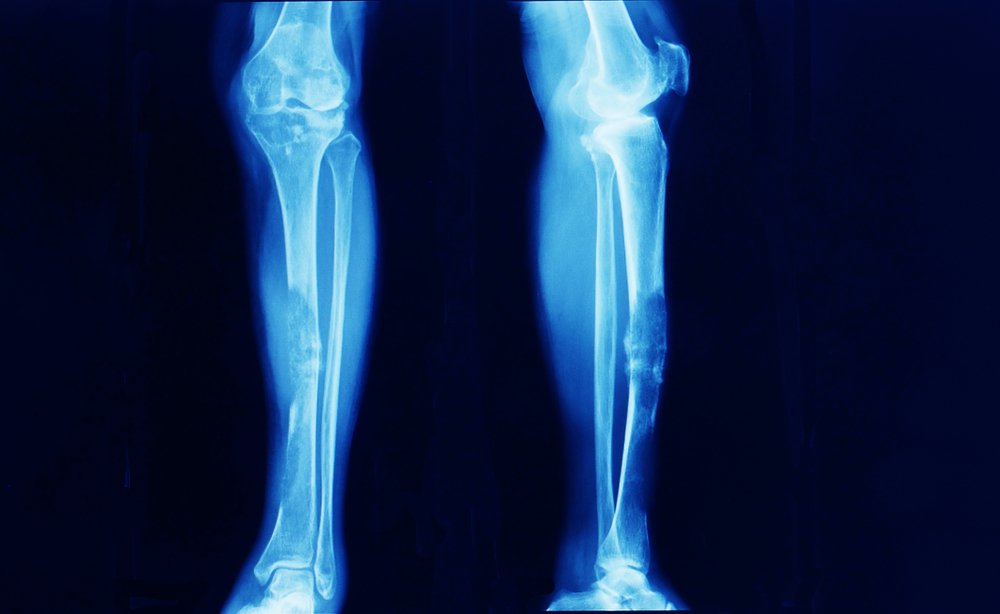
Radiological findings of Giant cell tumor:
1) An osteolytic area is seen near the epiphysis.
2) The cortex is expanded and thin.
3) There is no periosteal new bone formation.
4) Thin septa of bone traverse the interior and procedure a soap-bubble appearance.
5) The cortex may be disrupted in the late stages.
6) Joint extension is rear.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, 4th edition, P-632]

Investigation will you take in case of osteoclastoma:
i. Radiographs (X-ray) – destruction of bone substance,
ii. CT scan,
iii. MRI to determine the extent of tumor,
iv. Biopsy.
Treatment of Giant Cell Tumor:
A) Surgical methods:
Curettege and bone grafting: Enbloc excision: In whicg 2 cm of normal tissue is excised, Defects are filled with cancellous bone graft, freeze-dried allo0graft. Curettege and acrylic bone cementation: The hetat of polymerization destroy residual stromal and giant cell.
Curettege and cryiosurgery: This destroy the residual tumor at its margin of curettage by repetitive freezing thawing by liquid nitrogen.
Excision and reconstruction: After excision of the tumor one of the followings are followed, Turn o- plasty technique: After excision of the lower end of the femur, required length proximal tibia is choosen, Split into two halves and one halfs of its turned upside down and fixed with left over the stump of the femur.
- Arthrodesis
- Arthroplasty.
B) Radiotherapy.
C) Other methods:
1) Amputation.
2) Marginal resection with curettage.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, ” edition, P-633]
Differential diagnosis of giant cell tumor: Shortly remember by ‘BLUNACH”
- B-Benign chondroblastoma.
- L= Localized osteitis fibrosa.
- U- Unicameral bone cyst.
- N=Non-ossifying fibroma.
- A = Aneurysmal bone cyst
- C = Chondromyxoid fibroma.
- H=Hyperparathyroidism.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, ” edition.page-633]