Concept about Carditis – Health of the children has been considered as the vital importance to all societies because children are the basic resource for the future of humankind. Nursing care of children is concerned for both the health of the children and for the illnesses that affect their growth and development. The increasing complexity of medical and nursing science has created a need for special area of child care, i.e. pediatric nursing.
Pediatric nursing is the specialized area of nursing practice concerning the care of children during wellness and illness. It includes preventive, promotive, curative and rehabilitative care of children. It emphasizes on all round development of body, mind and spirit of the growing individual. Thus, pediatric nursing involves in giving assistance, care and support to the growing and developing children to achieve their individual potential for functioning with fullest capacity.
Concept about Carditis
Carditis:
Inflammation of the heart tissue or muscle tissue in the heart is called as carditis. Carditis is classified into three types:
- Endocarditis
- Myocarditis
- Pericarditis
Features of Carditis:
1. Endocarditis: Murmurs due to valvular involvement.
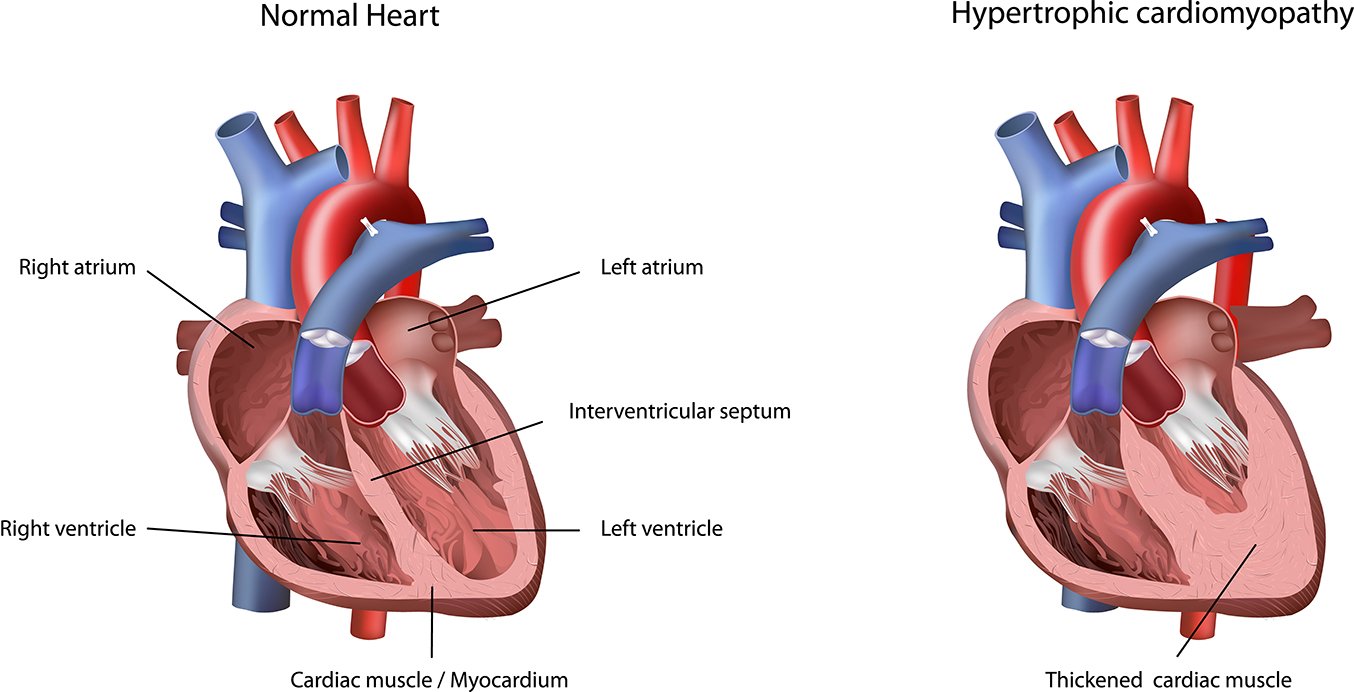
2. Myocarditis: Tachycardia, conduction defect, cardiomegaly.
3. Pericarditis: Pericardial rub & effusion.DAT
Results of Carditis:
Sometimes, carditis results in:
- Cardiomegaly &
- Congestive heart failure with pulmonary and systemic congestion.
Infective endocarditis is one of the most serious of all infections, which is due to microbial infection of a heart valve (native or prosthetic), the lining of the cardiac chamber (endocardium) or blood vessels (endothelium) or a congenital anomaly (e.g. septal defect) leading to the formation of bulky & friable vegetations laden with organisms.
Pathophysiology of infective endocarditis:
Endocardial damage by forceful jet of blood in pre-existing heart conditions.
↓
Deposition of platelet & fibrin within that damaged endothelium area & valve.
↓
Colonization of platelet & fibrin by micro-organism from the blood stream.
↓
Starts proliferation & produce vegetation.
↓
Pathological hall mark
Causes:
a. Bacteria:
i. Sreptococci:
- Streptococcus viridans
- Enterococci.
- Streptococcus bovis.
- Streptococcus pneumoniae.
- Others streptococcus
ii. Staphylococcus:
- Staphylococcus aureus. (Most)
- Staphylococcus epidermidis.
iii.Gram negative bacteria of HACEK group:
- H = Haemophilus
- A = Actinobacillus
- c = Cardiobacterium
- E = Eikenilla
- K = Kingella’
- iv. Anaerobes.
b. Others organism:
- Rickettsiae (Coxiella burnetii), fungi (Candida & aspergillus).
(Ref: Davidson 528 / (23)

Clinical diagnosis of infective endocarditis can be made on the presence of
- Two major criteria or
- One major & 3 minor criteria or
- Five minor criteria.
Modified Duke Criteria:
Major criteria –
Positive blood culture:
i. Typical organism from two culture
ii. Persistant positive blood culture taken > 12 hours apart.
iii. Three or positive cultures taken over >1 hour.
Endocardial involvement:
i. Positive echocardigraphic vegetations
ii. New valvular regurgitation
Minor criteria:
- Predisposing valvular or cardiac abnormality
- Intrarvenous drug misuse
- Pyrexia ≥38°C
- Embolic phenomenon
- Vasculitic phenomenon
- To gredie
- assige B
- Blood culture suggestive – organisms grown but not achieving major criteri
Definite infective endocarditis –
i. 2 major or
ii. 1 major +3 minor or
iii. 5 minor criteria
Possible infective endocarditis-
- One major + 1 minor criteria or
- 3 minor criteria
(Ref: Davidson-529/23)
Management of Infective Endocarditis:
Clinical features:
1. General features:
- Fever:
- Acute febrile illness in acute endocarditis.
- Persistent mild fever usually in sub-acute endocarditis.
- Unusual tiredness
- Night sweats.
- Weight loss
- Pallor
- Arthalgia.
ii. Cardiac features:
- Cardiac failure
- Conduction disorders eg. Heart block.
- Varying/changing murmurs:
- Appearance of new murmur eg. aortic regurgitation
- Change of pre-existing murmur.
iii. Spleen:
- Splenomegaly (usually when there is longer course).
- Tenderness & splenic rub may be present when there is infarction.
iv. Kidney:
- Loin pain
- Haematuria.
v. Embolic phenomenon:
- Cerebral emboli (Stroke)
- Systemic emboli
- Loss of pulses.
vi. Eye:
- Subconjunctival haemorrhage.
- Petechial hge on mucous membrane & fundi
vii. Hands and feet:
- Roth’s spot in fundi.
- Anaemia.
- Digital clubbing.
- Osler’s nodes on fingers
- Splinter haemorrhage
- Petechial rash
ii. Poor dentition.
Investigations:
i. Blood:
- Hb%- decreased (anaemia)
- Total count – Leukocytosis.
- Platelet count: decreased
- ESR & CRP – raised
- PBF: Normocytic normochromic anaemia
- Blood culture (key inv.) – More 3 to 6 sets of blood are collected at half an hour apart from different venepuncture sites before starting antibiotic and are sent for both aerobic & anaerobic culture.
ii. Urine for R/M/E: Proteinuria, hematuria.
iii. Chest X ray :
- Heart failure
- Cardiomegaly
iv. ECG:
- Conduction defect (AV block) due to abscess formation.
- MI due to embolic.
v. Echocardiography:
- Vegitations
- Valvular lesion
- Abscess.
Treatment:
a. Medical treatment:
i. Complete bed rest
ii. Removal of any source of infective focus e, g. dental root abscess.
iii. Antibiotics:
- Bactericidal antibiotic, should be given according to C/S at least 4 wks for native valve & 6 wks for prosthetic valve.
- Viridans Streptococcus / Streptococcus bovis:
✓ Benzyl penicillin IV & Gentamicin IV
Enterococci:
✓ Ampicillin sensitive Ampicillin IV & Gentamicin IV
✓ Ampicillin resistant Vancomycin IV & Gentamicin IV
S taphylococci:
✓ Penicillin sensitive Benzyl penicillin IV
✓ Penicillin resistant but Methicillin sensitive Flucloxacillin IV
Penicillin & Methicillin resistant Vancomycin IV & Gentamicin IV
iv. Treatment of complications
v. Monitoring of the pt.:
- Fever
- murmur-changing/not
- ESR
- C-reactive protein.
b. Surgical treatment:
- Cardiac surgery –Debridement of infected material & valve replacement

Indications:
- Heart failure due to valve damage.
- Failure of antibiotic therapy.
- Large vegetation on the left sided heart valves
- Abscess formation.
- Complication of infective endocarditis:
- (Ref-Davidson’s/234/-528-530)
- Heart failure due to valve damage.
Read more: