Concept about Thalassemia – Health of the children has been considered as the vital importance to all societies because children are the basic resource for the future of humankind. Nursing care of children is concerned for both the health of the children and for the illnesses that affect their growth and development. The increasing complexity of medical and nursing science has created a need for special area of child care, i.e. pediatric nursing.
Pediatric nursing is the specialized area of nursing practice concerning the care of children during wellness and illness. It includes preventive, promotive, curative and rehabilitative care of children. It emphasizes on all round development of body, mind and spirit of the growing individual. Thus, pediatric nursing involves in giving assistance, care and support to the growing and developing children to achieve their individual potential for functioning with fullest capacity.
Concept about Thalassemia
Definition:
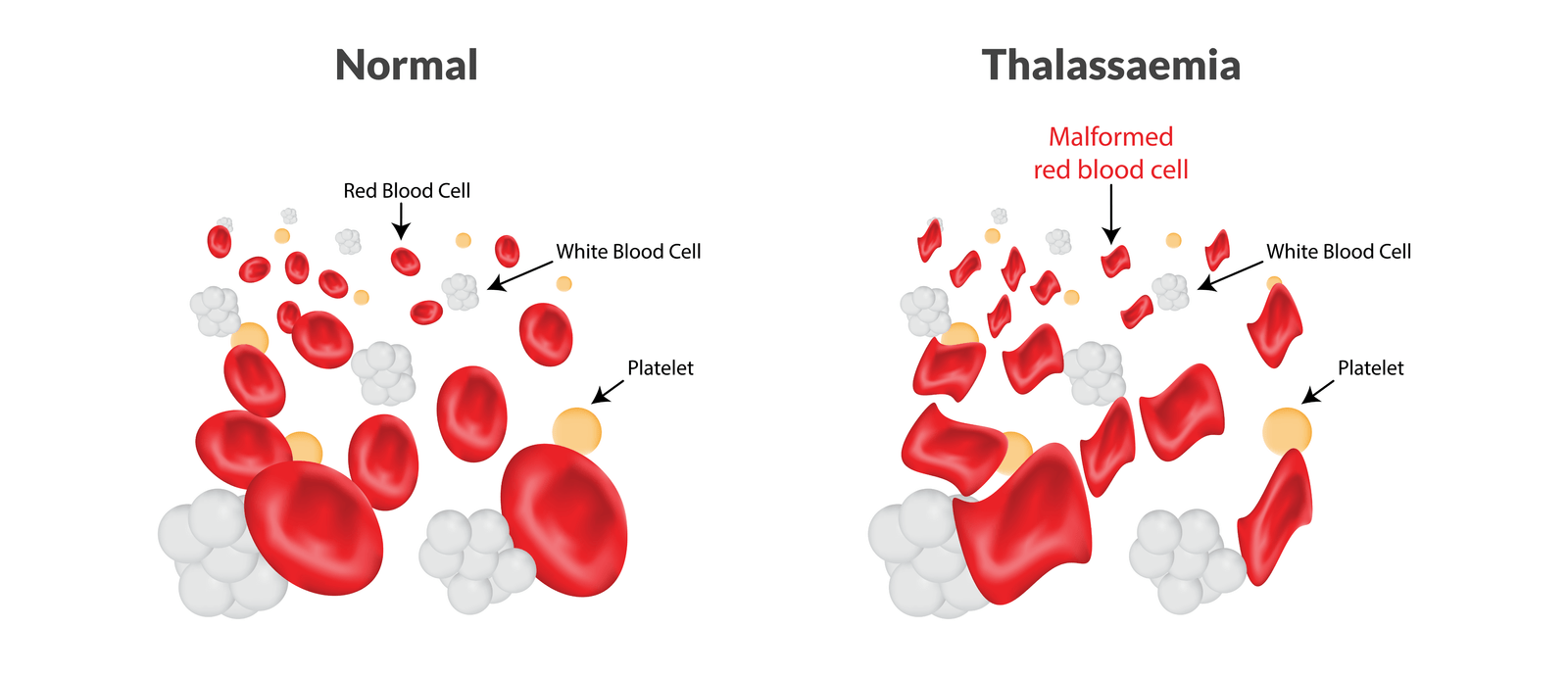
Thalassemia is a heterogeneous group of disorder, all are characterized by absence or decreased synthesis of a or ẞ chain of HbA
Or
Thalassemia is a group of hereditary hemolytic anemia characterized by reduction in the synthesis of hemoglobin.
(Ref: Paediatric Nursing, Parul Datta/34/324)
Classification:
A. On the basis of affected hemoglobin chain –
a) a-Thalassemia
b) B-Thalassemia
B. On the basis of clinical behavior both are divided as follows –
a) a-Thalassemia
- Silent carrier
- a-Thalassemia trait
- HbH disease
- Hydrops fetalis (Hb Bart)
b) B-Thalassemia –
- B-Thalassemia major (ẞ°)
- B-Thalassemia intermediate (B’)
- B-Thalassemia minor (β)
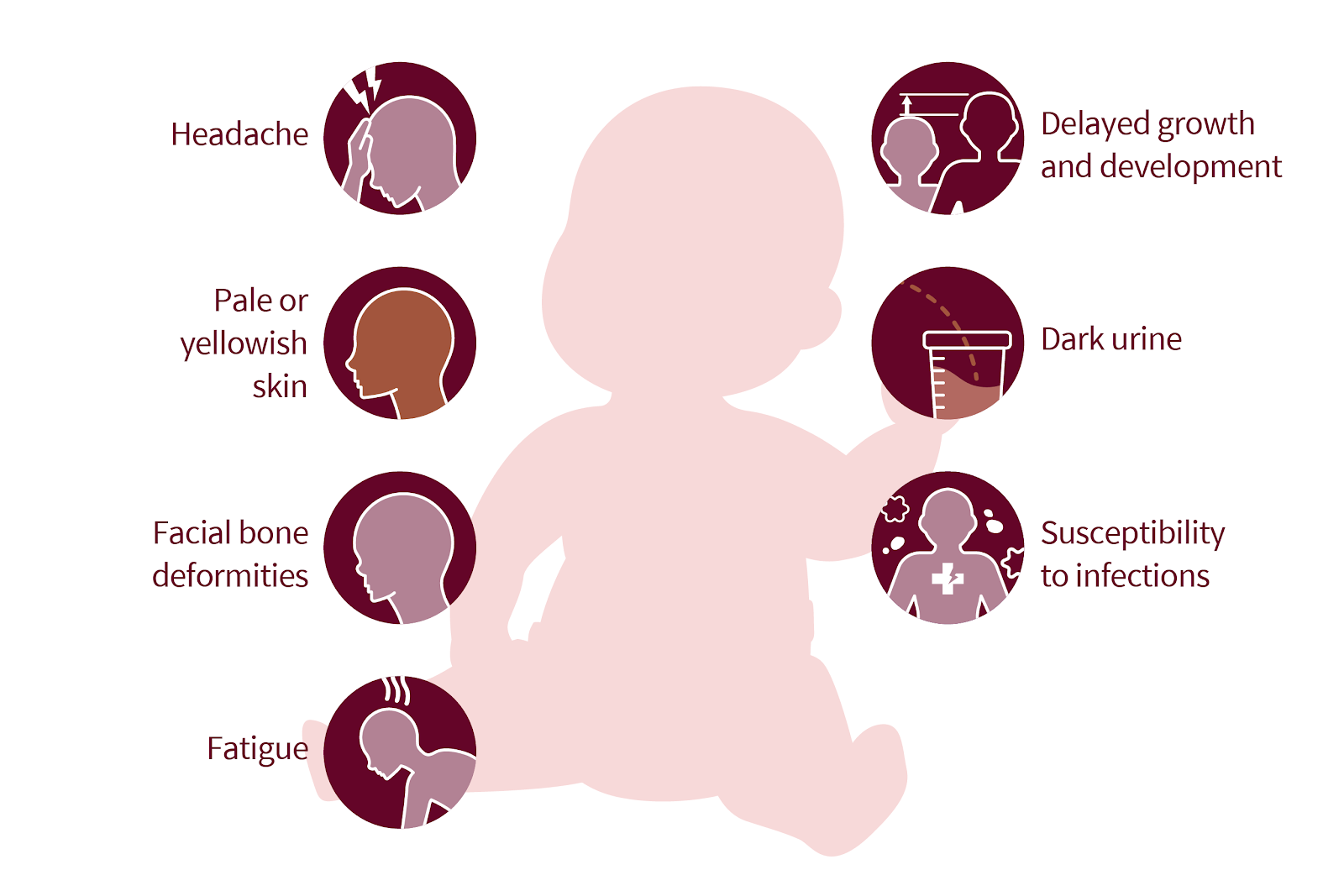
Clinical Features of Thalassemia:
a. Symptoms:
- Patient is usually child
- The child fails to thrive
- Patient is apathetic and allergic
- May complain of breathlessness at exercise
- May complain of anorexia, diarrhea, and recurrent fever.
- Lump in the left hypochondriac region
- Patient may show features of CCF
- Secondary sex characteristic may appear delayed
- If patient is in therapy, he/she may show the features of haemochromatosis
- H/O repeated blood transfusion and hospitalization
- Positive family history
- Growth retardation
b. Signs:
1. General examination:
Appearance: Thalassemia faces –
✓ Frontal bossing
✓ Malar prominence
✓ Depressed nasal bridge
✓ Mal-occlusion of mouth
✓ Parietal and frontal prominence
- Body built: short statured
- Anemia: Present
- Jaundice may be mild
- Skin may be pigmented
- Hair – Axillary, pubic hair may reduce
- Pulse – Rapid
II. Alimentary system: Splenomegaly, hepatomegaly

Treatment of Thalassemia:
1. Blood transfusion at regular interval
2. No iron therapy
3. If features of iron load found or after a reasonable period give desferrioxamine – SC by infusion pump for children 50-60 mg/kg/day for adults. 4. Vitamin C can be given which enhance iron excretion
5. Splenectomy if the enlarged spleen
6. Tab. folic acid 58 mg daily life long
7. Give proper Rx for infection and take prophylactic measures
8. If features of organ failure develop,, steps are taken accordingly
9. Bone marrow transplantation.ir
Diagnostic Evaluation of Thalassemia;
A. Blood examination shows the followings:
- Hemoglobin percentage-reduced usually 2 to 6 g/dl.
- RBC count reduced, 2 to 3 million/cmm.
- Fetal hemoglobin level (HbF) increased.
- Hematocrit values are reduced, MCV MCH, MCHC values are low
- Reticulocyte count increased or may be low.
- RBCs in peripheral smear shows-hypochromia, anisocytosis, poikilocytosis, microcytosis, nucleated RBCs and target cells.
- WBC count may be reduced or sometimes increased.
- Platelet count is usually normal or increased.
- Serum bilirubin level is moderately elevated.
- Serum iron level is high.
B. Bone marrow study shows hypercellular and erythroid hyperplasia.
C. Osmotic fragility test shows decreased fragility.
D. Radiological findings show skeletal changes including thinning of the cortex, widening of the If medulla and coarsening of trabeculations due to bone marrow hyperplasia in the long bones, metacarpals and metatarsals.
E. Skull bones show “hair-on-end” appearance due to vertical trabeculae or striations from widening of the diploic space and atrophy of the outer surface of the skull.
(Ref: Paediatric Nursing, Parul Datta/3/325)
Nursing Management of Thalassemia:
1. Assessment of child condition to prevent complications that can be done as hospital based or community based (at home).
2. Preparation for repeated hospitalization for treatment of the disease and its complications.
3. Arrangement of necessary diagnostic measures.
4. Administration of blood transfusion and iron chelating agent with appropriate precautions for specific therapy.
5. Provision of supportive care with rest, comfort, nutritious diet with restriction of iron containing food. Vitamin supplementation, immunization, hygienic care and other symptomatic care.
6. Prevention of infection by aseptic techniques and promotion of general cleanliness.
7. Preoperative and postoperative care during splenectomy with necessary health education after the surgery.
8. Information regarding treatment plan, prognosis and complications to be given to parent and family members with appropriate explanation.
9. Emotional support to the parents and family for effective coping about the stress of the illness.
10. Teaching the parent about importance of follow-up, blood transfusion, investigations, and signs of complications, dietary restriction, activity modification, recreation, diversion and available treatment facilities.
11. Referral and necessary guidance for available support services and community facilities. MIMAT-1
(Ref: Paediatric Nursing, Parul Datta/34/326)
Prevention of Thalassemia:
1. Antenatal screening in the first trimester of pregnancy by amniocentesis or chorionie villous sampling or fetoscopy help to detect thalassemia in fetal life.
2. Genetic counseling in that respect is very important preventive measure which guide the parent to decide whether to continue pregnancy with thalassemic fetus or to terminate pregnancy (by MTP) of affected fetus.
3. Carriers can be detected by simple blood examination or by identification of thalassemia
gene.
4. Creation of awareness among public regarding detection of thalassemia gene before marriage and marital counseling are also very important preventive aspect.
(Ref: Paediatric Nursing, Parul Datta/3/326)
Complications
Possible complications of thalassemia include:
- Iron overload.
- Infection.
In cases of severe thalassemia, the following complications can occur:
- Bone deformities.
- Enlarged spleen (splenomegaly).
- Slowed growth rates.
- Heart problems.
Read more: