
Concept about Steroids – This book covers the entire syllabus of “Pharmacology” prescribed by BNMC- for diploma in nursing science & midwifery students. We tried to accommodate the latest information and topics. This book is an examination setup according to the teachers’ lectures and examination questions.
At the end of the book, previous questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourish. The unique way of presentation may make your reading of the book a pleasurable experience.
Concept about Steroids
Basic concepts
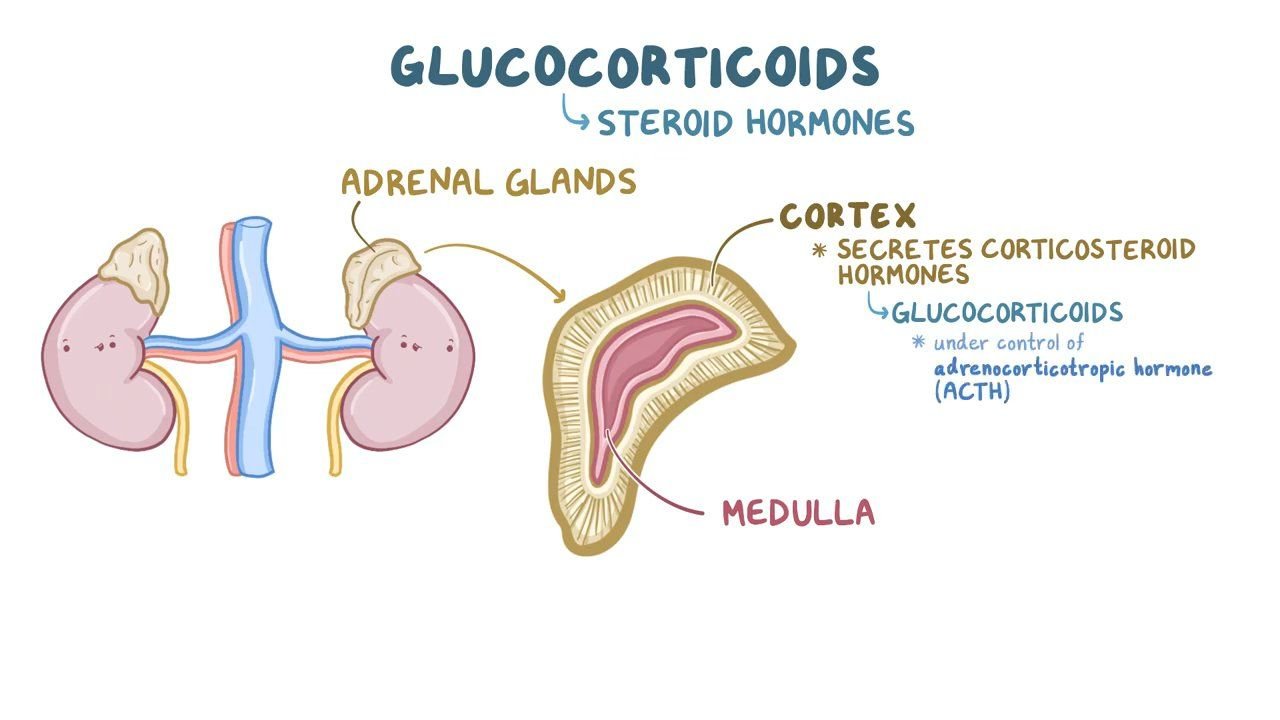
The adrenal cortex secretes several steroid hormones into the bloodstream. These are categorized by their actions into two main classes – mineralocorticoids and glucocorticoids. Aldosterone is the main mineral corticoid and is synthesized in the zona glomerulosa. It affects water and electrolyte balance, and possesses salt-retaining activity.
Hydrocortisone (cortisol) and cortisone are the main glucocorticoids and are synthesized in the zona fasciculata and zona reticularis. These affect carbohydrate, fat and protein metabolism, and suppress inflammatory and immune responses. Cortisol and cortisone also possess some mineralocorticoid activity.

The Adrenocortical hormones.
Small quantities of some sex steroids, mainly androgens, are also produced by the adrenal cortex.
Adrenocortical hormones are:
a. Mineralocorticoid.
1. Aldosterone.
2. Deoxycorticosterone.
b. Glucocorticoid.
1.Cortisol.
2. Corticosterone.
c. Androgen.
1.Dehydroepiandrosterone.
2. Androstenedione.
Adrenal cortex synthesize two types of steroids
a. The corticosteroids having 21 carbon atoms:
1. Glucocorticoids
2. Mineralocorticoids
b. Adrenal androgens having 19 carbon atoms
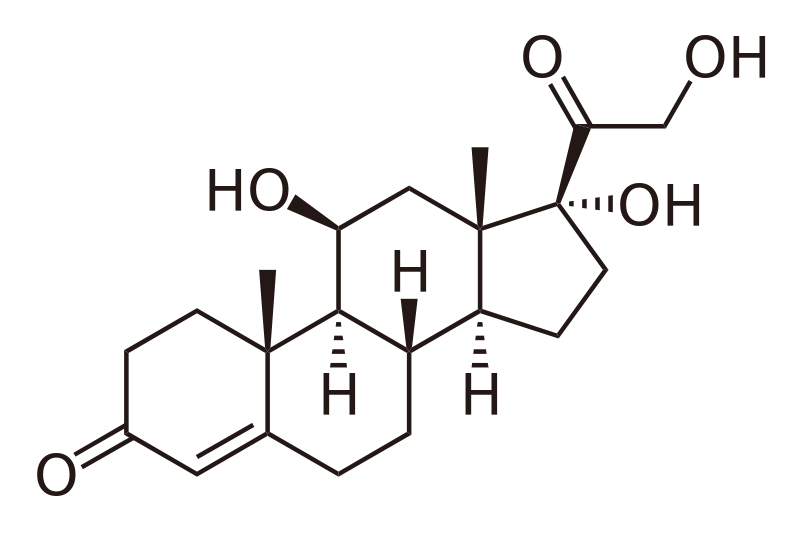
Chemistry of steroids
Steroids contain cyclopentanoperhydrophenantherene ring. All bear two carbon side chains at position C17, so that they have 21 carbon atoms in their molecules. The side includes a ketone group at position C2s which confers reducing properties of the molecules. There is an oxygen atom on carbon atom 3.
Glucocorticoids
The release of cortisol is controlled by negative feedback to the hypothalamic-pituitary-adrenal axis. There is a diurnal pattern of activity with an early morning peak in cortisol release. A variety of sensorineural inputs regulate the release of corticotrophin-releasing factor (CRF) in the hypothalamus; examples include physiological and psychological ‘stress’, injury and infection.
CRF, a 41-amino-acid polypeptide, reaches the anterior pituitary in the hypothalamo- hypophysial portal system where it stimulates the release of adrenocorticotrophic hormone (ACTH). ACTH is formed from a larger molecule, pro-opiomelanocortin, and is released into the circulation where it stimulates the synthesis and release of cortisol from the adrenal cortex. Natural and artificial glucocorticoids circulating in the blood exert a negative feedback effect on the production of both CRH and ACTH.
Biosynthesis of adrenocortical hormone:
Site: Mitochondria & endoplasmic reticulum of adrenocortical cells.
Precursor: Cholesterol.
The Classification of Glucocorticoids.
According to the duration of action
A. Short acting (8-12 hours)
1. Cortisol
2. Cortisone
3. Corticosterone
4. Fludrocortisone
B. Intermediate acting (12-36 hours)
1. Prednisone
2. Prednisolone
3. 6g-methylprednisolone
4. Triamcinolone
B. Long acting (36-72 hours)
1. Dexamethasone
2. Betamethasone
3. Paramethasone
Mechanism of action of corticosteroids
Endogenous and synthetic corticosteroids act in a similar way. The hormone or drug circulates to peripheral tissues where it enters cells (steroids are lipid soluble) and binds to cytosolic corticosteroid receptors. After hormone binding, these receptors are translocated to the nucleus where they interact with DNA and lead to the transcription of corticosteroid-responsive genes (CRG).
The products of these CRGs have diverse effects on the target tissues. The actions of corticosteroids are divided into effects on inorganic metabolism (mineralocorticoid effects) and effects on organic metabolism (glucocorticoid effects).
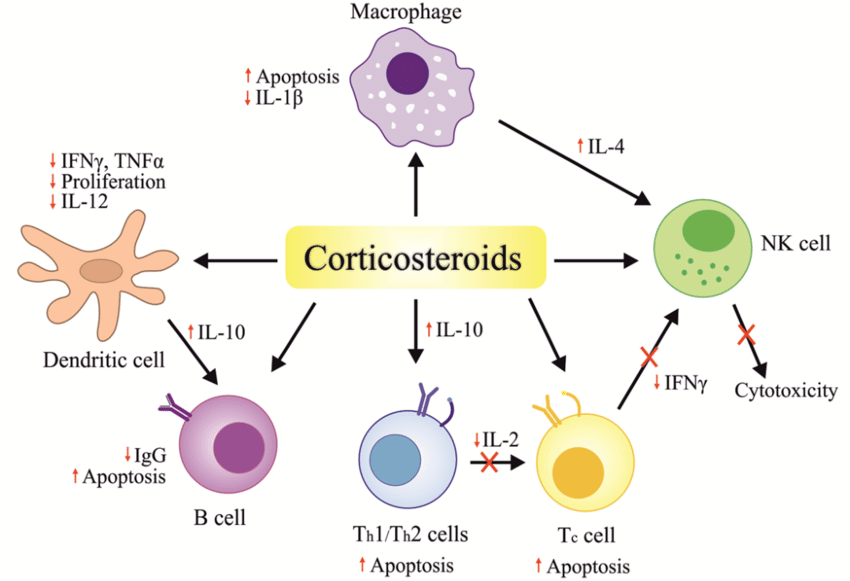
Action of glucocorticoids
Anti-inflammatory actions
1. Suppress migration of leukocytes to the inflamed area.
2. Suppress reparative process and function of fibroblast.
3. Reverses the enhanced capillary permeability.
4. Stabilizes the lysosomal membrane.
5. Inhibits phospholipase-A2, thereby block synthesis of prostaglandin and leukotrines.
6. Sequestered lymphocytes in spleen, lymph node and bone marrow.
7. Release the adherent factor of vascular endothelium.
8. Reduce the action of cytokinin.
Effects of cortisol/glucocorticoids:
Metabolic effects:
On carbohydrate metabolism: Cortisol shows anabolic effects. It increases blood glucose level by
- Gluconeogenesis.
- Glycogenolysis.
- Glycogenesis.
- Peripheral utilization of glucose.
- Transport of glucose into the cells.
On protein metabolism: Cortisol shows catabolic effect and it causes reduction of protein stores of all the cells of the body except liver. So, though the protein stores are reduced elsewhere in the body, the liver proteins become enhanced. Cortisol causes –
- Decrease Protein synthesis in peripheral tissues other than liver.
- Catabolism of protein in peripheral tissues.
- Synthesis of plasma proteins by the liver.
- Mobilizes amino acids from non-hepatic tissue and thereby tissue protein stores.
- Plasma amino acid concentration
On fat metabolism:
- Fatty acid mobilization from the adipose tissue and thereby plasma free fatty acid concentration.
- Fatty acid utilization for energy.
- Lipolysis.
- Ketone bodies formation.
- Excess cortisol causes deposition of fat in the chest region of the body which looks like a ‘Buffalo hump’ as well as in the head region looks like a ‘Moon face’.
Anti-allergic effects: It inhibits the release of chemical mediators (e.g. histamin) that causes inflammation.
Indications of corticosteroid
Corticosteroids have wide-ranging and powerful effects on human physiology. There are two main areas where these properties are taken advantage of in the therapeutic use of corticosteroids – physiological replacement therapy of corticosteroid deficiency, and anti-inflammatory therapy and immunosuppression.
| Replacement therapy |
|
| Allergic reactions |
|
| Collagen-vascular disorders |
|
| Eye diseases |
|
| Gastrointestinal diseases |
|
| Hematologic disorders |
|
| Systemic inflammation |
|
| Infections |
|
| Inflammatory conditions of bones and joints |
|
| Nausea and vomiting |
|
| Neurologic disorders |
|
| Organ transplants |
|
| Pulmonary diseases |
|
| Renal disorders |
|
| Skin diseases |
|
| Thyroid diseases |
|
| Miscellaneous |
|
Adverse effects:
These are extensions of the pharmacological action which become prominent with prolonged therapy, and are a great limitation to the use of corticoids in chronic diseases.
1. Cushing’s habitus: characteristic appearance with rounded face, narrow mouth, supraclavicular hump, obesity of trunk with relatively thin limbs.
2. Fragile skin, purple striae-typically on thighs and lower abdomen, easy bruising, telangiectasis, hirsutism. Cutaneous atrophy localized to the site occurs with topical application as well.
3. Hyperglycaemia, may be glycosuria, precipitation of diabetes.
4. Muscular weakness: proximal (shoulder, arm, pelvis, thigh) muscles are primarily affected. Myopathy occurs occasionally, warrants withdrawal of the corticoids.
5. Susceptibility to infection: this is nonspecific for all types of pathogenic organisms. Latent tuberculosis may flare; opportunistic infections with low grade pathogens (Candida, etc.) set in.
6. Delayed healing: of wounds and surgical incisions.
7. Peptic ulceration: risk is doubled; bleeding and silent perforation of ulcers may occur. Dyspeptic symptoms are frequent with high dose therapy.
8. Osteoporosis: Posterior subcapsular cataract may develop after several years of use, especially in children.
9. Glaucoma: may develop in susceptible individuals after prolonged topical therapy.
10. Growth retardation: in children occurs even with small doses if given for long periods.
11. Foetal abnormalities: Cleft palate and other defects are produced in animals, but have not been encountered on clinical use in pregnant women.
12. Psychiatric disturbances: mild euphoria frequently accompanies high dose steroid treatment.
The Contraindications and Precautions of steroid therapy
Contraindications:
The following diseases are aggravated by corticosteroids. Since corticosteroids may have to be used as a life-saving measure, all of these are relative contraindications in the presence of which these drugs are to be employed only under compelling circumstances and with due precautions.
A. Peptic ulcer
B. Diabetes mellitus
C. Hypertension
D. Viral and fungal infections
E. Tuberculosis and other infections
F. Osteoporosis
G. Herpes simplex keratitis
H. Psychosis
I. Epilepsy
J. CHF
K. Renal failure
Precautions of steroid therapy:
1. Exclude any contraindication if therapy is indicated for more than week.
2. Measure blood pressure regularly.
3. Estimate blood sugar level weekly.
4. X-ray vertebral column to see any osteoporesis lesion.
5. Avoid sudden withdrawal of therapy.
6. Maintain a gradual tapering dose during withdrawal of the therapy
Withdrawal of steroid therapy
In clinical practice withdrawal of steroid therapy is an important understanding regarding the duration of steroid therapy. The use of corticosteroids for days or a few weeks (short course) dose not lead to adrenal insufficiency; therefore no need to gradual withdrawal of the drug. Acute adrenal insufficiency results from too rapid withdrawal of corticosteroids after prolong therapy therefore gradual withdrawal is necessary.
Effects of sudden withdrawal of steroid therapy:
1. Adrenocortical insufficiency
2. Weight loss
3. Arthalgia
4. Itchy skin nodule
5. Conjunctivitis.
6. Rhinitis
Anabolic sterolds
The steroids, which stimulate anabolism rather than catabolisrn in the body as a whole, are called anabolic steroids.
Name of anabolic steroids;
a. Oral use:
1. Ethylesternol
2. Oxandrolone
3. Oxymethone
4. Stanozolol
5. Norethandrolone
b. Intramuscular use:
1. Nandrolonephenpropionate
2. Nandrolone decanoate
3. Nor-ethandrolone

Indications of anabolic steroids
1. Osteoporosis
2. Retarded growth
3. Acute renal failure
4. General wasting conditions
5. Aplastic anaemia
6. Hereditary angioedema
7. Itching of biliary obsffuction.
8. Various condition in which negative nitrogen balance exists
Disadvantages:
1. Na+-retention, masculinisation of foetus
2. Aggravation of carcinoma of prostate
3. Premature epiphyseal closure
4. Cholestatic jaundice
Diabetes Mellitus & Anti Diabetic Drugs
Diabetes mellitus
It is a clinical syndrome characterized by hyperglycaemia due to absolute or relative deficiency of insulin.
Therapeutic classification of Diabetes Mellitus:
Type-I Diabetes (IDDM):
Insulin dependent diabetes mellitus, is a severe form associated with ketosis in untreated state and occurs most commonly in Juveniles but occasionally in adults, specially the non-obese. It is a catabolic disorder in which circulating insulin is virtually absent; plasma glucagon is elevated, and the pancreatic B-cells fail to respond to all insulinogenic stimuli. Exogenous insulin is therefore required.
Type-II Diabetes (NIDDM):
Non-insulin dependent diabetes mellitus, represents a heterogenous group comprising milder forms of Diabetes that occurs predominantly in adult and occasionally in adolescent. Circulating endogenous insulin is sufficient to prevent ketoacidosis but is often either subnormal relatively inadequate because of tissue insensitivity.
MRDM: Malnutrition related diabetes mellitus.
GDM: Gestational diabetes mellitus.
Other types: Associated with certain disease and syndrome.
Post prandial blood glucose level (mmol/L)
4-7:Normal
>7-10: Suggestive of diabetes
> 10: Almost certainly diabetes
Fasting blood glucose level (mmol/L)
4- 6: Normal
>6-8: Suggestive of diabetes.
>10; Almost certainly diabetes
IDDM Vs NIDDM:
| Points | IDDM | NIDDM |
| Type | Type-I | Type-II |
| Age of onset | Juvenile onset <30y | Adult onset >40y |
| Body weight | Normal/low | Obese (50-90%) |
| Ketonuria | Common | No |
| Endogenous insulin | Severe deficiency | Moderate deficiency |
| Insulin resistence | Occasional | Always |
| Islets cell antibody | Present | Absent |
| Family h/o diabetes | No | Present |
| Treatment with insulin | Always necessary | Not always required |