Destructive operations – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Destructive operations
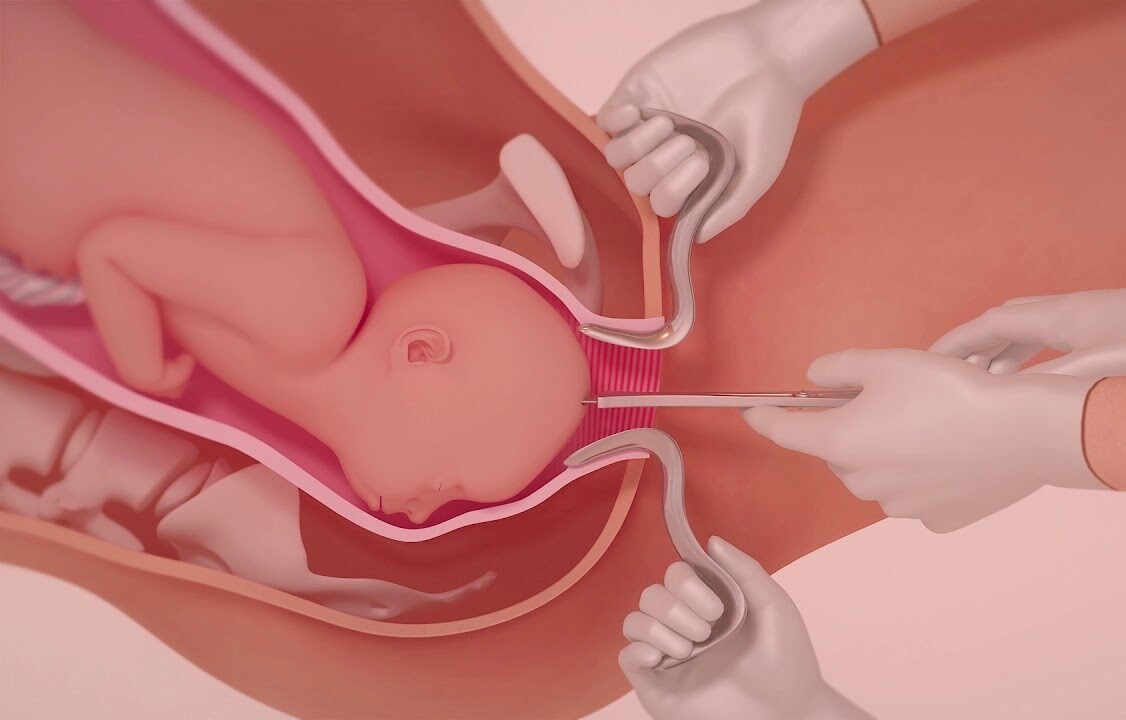
Destructive operations in obstetrics:
1. Craniotomy
2. Decapitation
3. Evisceration/embryotomy.
4. Cleidotomy.
[Ref-D. C. Dutta’s Obs/9/5431]
Indications of craniotomy:
1. Neglected obstructed labour: Dead fetus with cephalic presentation (vertex, face & brow) producing obstructed labour.
2. Hydrocephalus even with a living fetus.
3. Interlocking head of twins.
4. Arrested after-coming head in breech delivery.
[Ref-D. C. Dutta’s Obs/9/543]
Post-operative management following destructive operations:
1. Mental support and reassurance.
2. To exclude rupture of uterus or laceration on the genitalia exploration of utero vaginal canal must be done.
3. Catheterization for 3-5 days after operation.
4. Adequate 1/V fluid.
5. Blood transfusion if needed.
6. Antibiotic.
7. Sedative can be given.
[Ref-D. C. Dutta’s Obs/9/545]
Complications of destructive operations:
1. Injury:
a. Injury to the utero-vaginal canal.
b. Rupture of the uterus.
c. Injury to the adjacent viscera (e.g. urinary bladder, rectal wall etc.)
2.Post-partum haemorrhage hypovolaemia&dehydration-shock.
3. Puerperal pyrexia.
4. Puerperal sepsis.
5. Subinvolution.
6. Vesico-vaginal fistula.
7. Recto-vaginal fistula (rarely).
[Ref-D. C. Dutta’s Obs/9/545]

Decapitation:
It is a destructive operation whereby the fetal head is severed from the trunk & the delivery is completed with the extraction of the trunk & that of the decapitated head per-vagina.
Indications of decapitation:
- Neglected shoulder presentation with dead fetus.
- Interlocking head of twins.
[Ref-D. C. Dutta’s Obs/9/545]
Definition of Version
Version:
It is a manipulative procedure designed to change the tie or to bring the comparatively favourable pole to the lower pole of the uterus.
[Ref-D. C. Dutta’s Ohs/9/541]
Types of version:
- Internal
- External
- Bipolar (Braxton-Hicks) version.
[Ref-D. C. Dutta’s Obs/9/541]
External cephalic version:
It is done to bring the favourable cephalic pole in the lower pole of the uterus.
[Ref-D. C. Dutta’s Obs/9/541]
Indication of external cephalic version:
- Breech presentation.
- Transverse lie.
[Ref-D. C. Dutta’s Obs/9/541]
Contraindications of external cephalic version:
1. Antepartum haemorrhage:
a. Placenta praevia.
b. Abruptio placenta.
2. Risk of placental separation – antepartum haemorrhage.
3. Fetal causes:
a. Major congenital anomalies.
b. Dead fetus.
c. Hyperextension of the head.
d. IUGR.
4. Multiple pregnancy.
5. Ruptured membranes with drainage of liquor.
6. Known congenital malformations of uterus.
7. Contracted pelvis.
8. Previous caesarean delivery (risk of scar rupture)
9. Obstetric complications:
a. Severe pre-eclampsia.
b. Eclampsia
c. Obesity.
d. Elderly primigravidae.