Rupture Of The Uterus- This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Rupture Of The Uterus
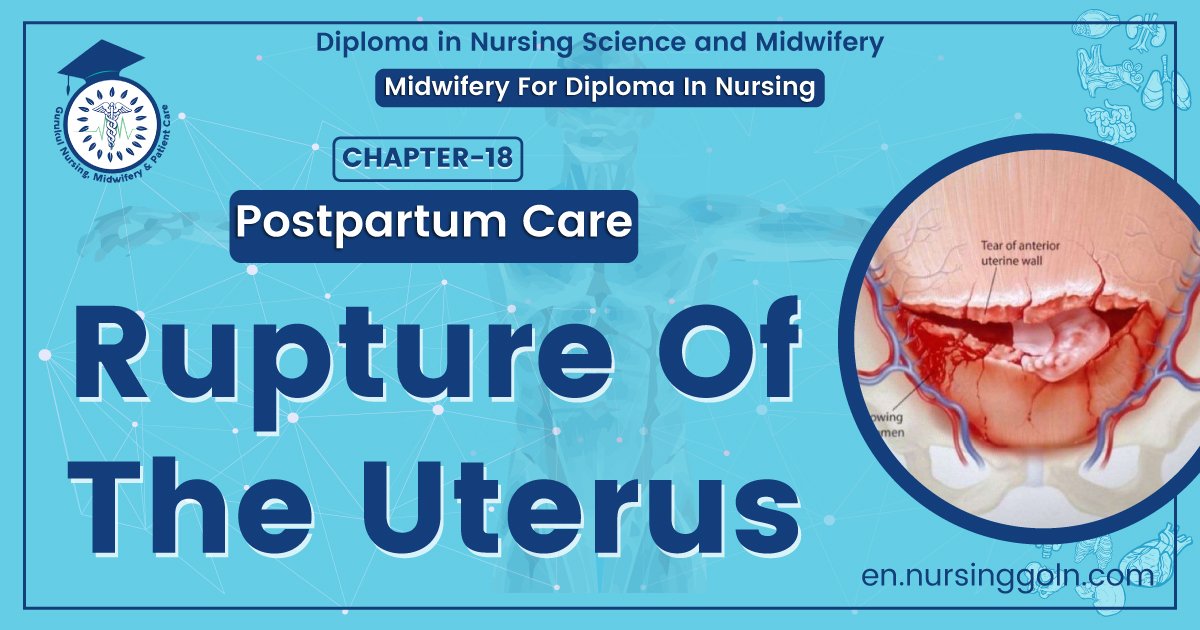
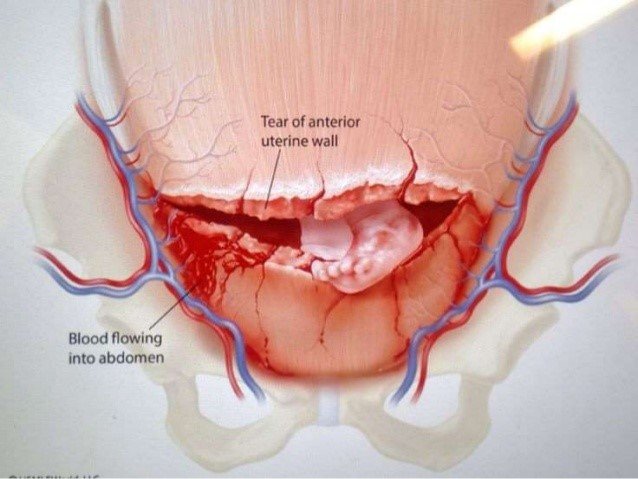
Rupture of the uterus
Dissolution in the continuit of the uterine wall an) time beyond 28 weeks of pregnancy is called rupture of the uterus.
Types:
1. Complete.
2. Incomplete.
Causes of rupture of the uterus
1. Causes of spontaneous rupture of uterus
During pregnancy: The causes are –
- Weakening of the uterine walls following dilatation and curettage operation ormanual removal of placenta.
- The weakening of the uterine walls results from fibrosis out of bruising, stretchingor tearing of the uterine muscles in previous labours.
- Congenital malformation of the uterus (bicornuate variety).
- In couvelaire uterus.
During labour
- Obstructed labour.
- Grand multipara.
2. Causes of scar rupture: During pregnancy:
- The weakening of such scar is due to implantation of the placenta over the scar and consequent increased vascularity.
- Injudicious administration of oxytocin.
- Use of prostaglandin for inducting of abortion or labour.
- Forcible external version specially under general anesthesia κ
- Fall or blow on the abdomen.
During labour
- The classical or hysterotomy scar is more vulnerable to rupture during labour.
- Internal podalic version-specially following obstructed labour.
✓ Destructive operation.
✓ Manual removal of placenta.
✓ Application of forceps or breech extraction through incompletely dilated cervix.
✓ Injudicious administration of oxytocin for augmentation of labour.
3. latrogenic or traumatic.
Diagnosis
Clinically:
✓There is a sense of something giving way at the height of uterine contraction.
✓ The constant pain is changed to dull aching pain with cessation of uterine contractions.
✓ General examination reveals features of exhaustion and shock.
✓ Abdominal examination revealsSuperficial fetal, parts.
✓Absence of F.H.S.
✓ Absence of uterine contour.
✓ Two separate swelling one contracted uterus and the other-fetal ovoid.
✓ Vaginal examination reveals.
- Recession of the presenting part and
- Varying degrees of bleeding.
Treatment
1. Resuscitation of the patient
2. Laparotomy: Any of the three procedures may be adopted following laparotomy –
A. Hysterectomy:
- Hysterectomy is the surgery for rupture uterus unless there is sufficient reason to preserve. This is specially indicated in spontaneous obstructive rupture.
- It is preferable to perform a quick subtotal hysterectomy, rather than total hysterectomy.
B. Repair
- This is mostly applicable to a scar rupture where the margin-, are clean, Repair is done by excision of the fibrous tissue at the margins.
B. Repair and sterilization: This is mostly done in patients with a clean cut scar rupture having desired number of children.
Nursing Management
A. Monitor for the possibility of uterine rupture.
- In the presence of predisposing factors, monitor maternal labor pattern closely for hypertonicity or signs of weakening uterine muscle.
- Recognize signs of impending rupture, immediately notify the physician, and call for assistance.
B. Assist with rapid intervention.
- If the client has signs of possible uterine rupture, vaginal delivery is generally not attempted.
- If symptoms are not severe, an emergency cesarean delivery may be attempted and the uterine tear repaired.
- If symptoms are severe, emergency laparotomy is performed to attempt immediate delivery of the fetus and hen establish homeostasis.
- Implement the following preparations for surgery.
✓Monitor maternal blood pressure, pulse, and respirations; also monitor fetal heart tones.
✓ If the client has a central venous pressure catheter in place, monitor pressure to evaluate blood loss and effects of fluid and blood replacement.
✓ Insert a urinary catheter for precise determinations of fluid balance.
✓ Obtain blood to assess possible acidosis.
✓ Administer oxygen, and maintain a patent airway.

C. Prevent and manage complications. Take these steps in order to prevent or limit hypovolemic shock:
- Oxygenate by providing 8 to 10 L/min using a closed mask.
- Restore circulating volume using one or more IV lines. Evaluate the cause, response to therapy, and fetal condition.
- Remedy the problem by preparing the client for surgery and administering antibiotics.
D. Provide physical and emotional support.
- Provide support for the client’s partner and family members once surgery has begun.
- Inform the partner and family how they will receive information about the mother and newborn and where to wait.