
Anorectal malformation/Imperforated anus mean – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Anorectal malformation/Imperforated anus mean
Anorectal malformation
Anorectal malformations (ARMs) are developmental deformities of the lower end of the alimentary tract, i.e. the anorectal canal.
Or
Anorectal malformations are birth defects, or problems that happen as an unborn baby is developing during pregnancy.
Or
Anorectal malformations, also known as imperforate anus, are defects that occur during the fifth to seventh weeks of fetal development.
Imperforated anus
The term imperforate anus is used to describe all congenital abnormalities of the anorectal canal or in location of the anus within the perineum.
Or
A birth defect in which the rectum is a blind alley and there is no anus. Imperforate anus occurs in about 1 in 5,000 births, and it can be corrected by surgery.

Fig: Imperforated anus
Causes of imperforate anus
1. The exact cause of these malformations is not known.
2. It occurs due to arrest in embryonic development of the anus, lower rectum and urogenital tract at the 5th week of embryonic life.
Associated anomalies of imperforated anus
- Anal fissure: It is the most frequent cause of fresh rectal bleeding and usually follows a tear or small laceration of the mucocutaneous junction of the anus during passage of a hard fecal matter in a severely constipated child.
- Perianal abscess and fistula
Classification of ano-rectal malformations
A. Classification of ARMs can be done into three groups in the infants without a normal anus.
1. With a visible abnormal opening of the bowel:
- Anal stenosis
- Anoperineal fistula.
- Anovestibular fistula in female.
2. With an invisible but manifested opening of the bowel:
- Rectovaginal fistula in female.
- Rectourethral fistula in male,
- Rectovesicular fistula.
3. No manifested opening of the bowel:
- Persistent anal membrane.
- Rectal atresia.
B. Anorectal malformations can be classified into two groups on the basis of levatorani muscle, which is the main muscle of fecal control-
1. Supralevator or high ahorectal malformations: When rectum terminates above the levatorani muscle, which is found as rectal atresia, rectoprostatic fistula and rectovaginal fistula. About 30 percent of children with high ARMs or associated genito-urinary fistula achieve bowel continence.
2. Transleuator or low anorectal malformations: When rectum terminates below the levatorani muscle, e.g. in anocutaneous fistula and anovestibular fistula. About 90 percent of children with low ARMs achieve bowel continence.
Clinical features of anorectal malformation
Management of ARM
- The reconstructive surgery is done to correct or repair the congenital malformations. It depends upon the type of anomalies and sex of the infant
- In case of low ARM; rectal cutback anoplasty or Y-V plasty is done for male infants and dilatation of fistula with definitive repair or perineal anoplasty is performed for female infant.
- In case of high ARMs, initial colostomy is done in the neonatal period followed by definitive reconstructive surgery.
- Colostomy closure is done after 10-12 weeks of surgery.
Nursing management of ARMS
Neonatal conditions requiring surgery fall into twomain categories –
- Those which are life-threatening & need immediate surgery.
- Those which may be postpone until the baby is in the optimum condition for surgery.
Much of the preoperative care will be specific to the condition, but the general principles are as follows-
Preoperative care:
1. Stabilize temperature: Maintenance of warm, prevention of hypothermia & hyperthermia & prevention of heat loss.
2. Stabilize respiratory state: Correct acidosis or electrolytes imbalance & Oz therapy.
3. Ensure good hydration with the administration of IV fluid.
4. Screen for infections & begin antibiotics
5. Check consent forms are signed & contact telephone number obtained from the Parents
6. Encourage the parents to touch or cuddle their baby before surgery.
Postoperative care:
1. Promote a good recovery.
2. Identify & treat complications early
3. Prevent infections
4. Prevention of skin breakdown around colostomy wound
5. Routine postoperative care to be provided after colostomy & definitive surgery.
6. Established adequate nutrition
7. Ensure the baby is free from pain & discomfort
8. Promote parental involvement & interaction
9. Emotional support for family copying & demonstrate colostomy care
10. Health education to be given about continuation of care at home, diet modification, bowel habit & need for medical help.
Complications of ARMs
The common complications of ARMs are –
1. Urinary tract infection (UTI).
2. Intestinal obstruction.
3. Fecal impaction.
4. Colostomy related problems.
5. Recurrence of fistula.
6. Anal stenosis and
7. Postoperative complications.
Associate anomalies of imperforate anus
In case of imperforate anus associated anomalies are expressed by acronym – VACTERL
| V | Vertebral anomalies |
| A | Anal atresia |
| C | Cardiovascular anomalies |
| T | Tracheo esophageal fistula |
| E | Esophageal atresia |
| R | Renal anomalies |
| L | Limbs defects |
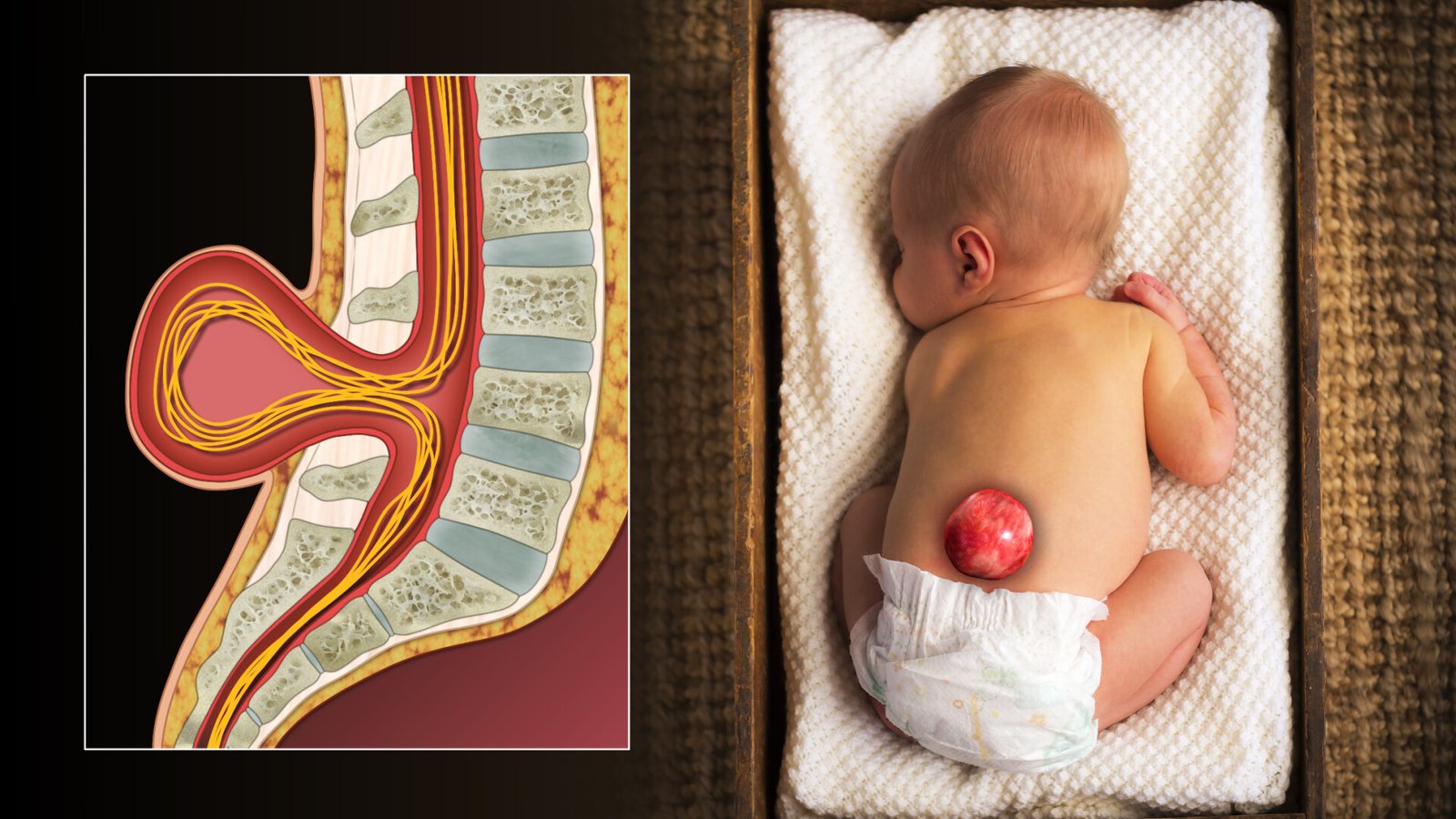
Spina bifida
It is the congenital defect of the spinal column due to failure of the fusion of vertebral arches with or without protrusion of the meninges and dysplasia of the spinal cord.
Or
Spina bifida is a type of birth defect called a neural tube defect. It occurs when the bones of the spine (vertebrae) don’t form properly around part of the baby’s spinal cord. Spina bifida can be mild or severe. The mild form is the most common. It usually doesn’t cause problems or need treatment.
Classification of spina bifida
1. Spina bifida cystica
2. Spina bifida occulta
Clinical features of spina bifida
Most of the cases are asymptomatic. Some children present with –
1. Cutaneous lesions over the defect
2. Tuft of hairs, nevus, lipoma, hemangioma, dermal sinus or as dimple in the skin
3. There may be intraspinal lesions like dermoid cyst, intramedullary lipoma, etc.
Symptomatic children present with –
1. Progressive deformity of the foot
2. Changes in micturition pattern
3. Alteration in the gait
4. Trophic ulcers on the toes and feet.
5. Other significant anomalies of the spinal cord (syringomyelia, diastematomyelia, tethered cord, etc.)
Management of spina bifida
1. Progressive neurological deficits require surgical correction of the defect.
2. Laminectomy is done and the intraspinal lesion is excised.
3. Operation can be done even before neurological deficit appears in selected cases.
4. Myelo-CT scan and MRI help to confirm the diagnosis before operation.