Bowel Intestinal Obstruction – This course is designed to understand the concept of community health nursing: nurses’ roles and interventions in family health, school health, occupational health, environmental health, elderly health care, gender issues, disaster management and principles and terminology of epidemiology. The aim of the course is to acquire knowledge and skills in community health nursing.
Bowel Intestinal Obstruction
Definition of Bowel Intestinal Obstruction:
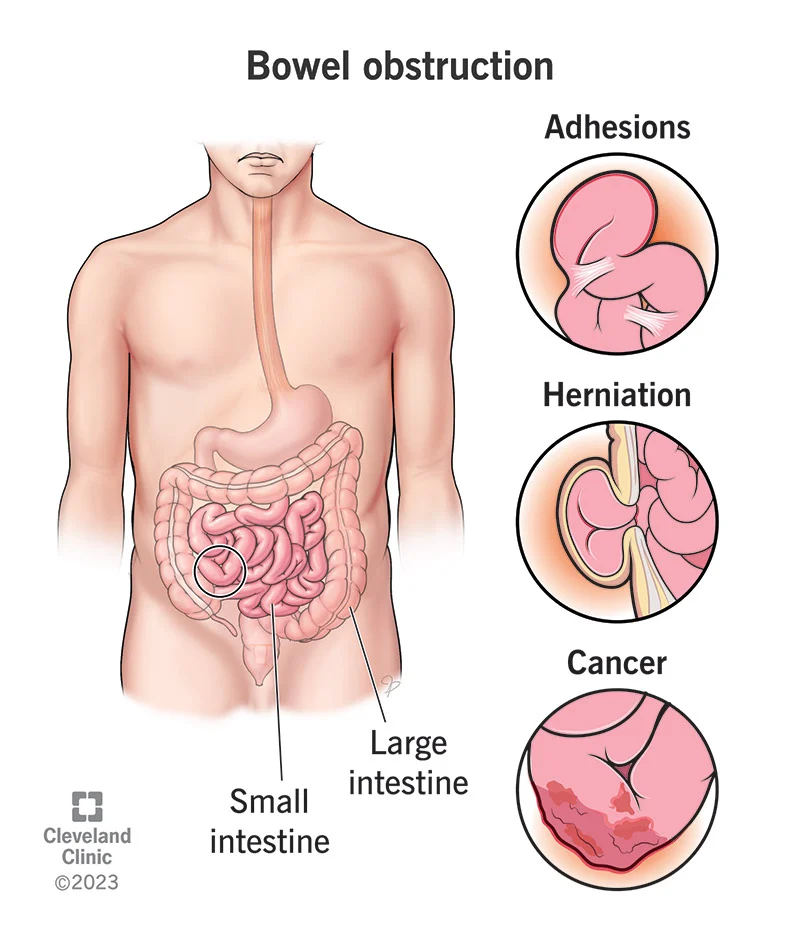
Bowel obstruction, also known as intestinal obstruction, is a mechanical or functional obstruction of the intestines which prevents the normal movement of the products of digestion. Either the small bowel or large bowel may be affected. Signs and symptoms include abdominal pain, vomiting, bloating and not passing gas
Or,
Intestinal obstruction is a blockage that keeps food or liquid from passing through the small intestine or large intestine (colon).
Or,
Intestinal obstruction is an interruption in the normal forward flow of intestinal content along the intestinal tract.
Causes of Intestinal Obstruction:
A. Dynamic (mechanical):
a. Intra-luminal:
- Fecal impaction
- Bezoar
- Gallstone
- Parasites eg. round worm
- Foreign bodies eg. marbles
b. Intra-mural:
- Stricture
- Malignancy
e. Extra-mural:
- Bands/adhesions
- Hernias
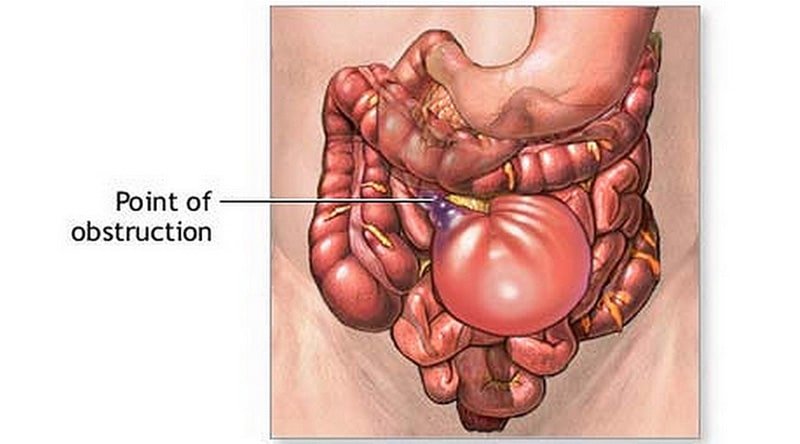
- Volvulus
- Intussusception
B. Adynamic:
a) Paralytic ileus
b) Mesenteric vascular occlusion
c) Pseudo obstruction
Classification of Intestinal Obstruction:
A. According to the level of obstruction:
a) Large gut obstruction
b) Small gut obstruction:
✔ Upper small gut obstruction
✔ Middle small gut obstruction
✔ Lower small gut obstruction
B. On the basis of nature of presentation:
a) Acute obstruction-usually in small intestine
b) Sub-acute
c) Chronic obstruction-usually in large intestine
d) Acute or chronic-Which spread from large gut to small gut
C. According to the state of peristalsis:
a) Dynamic (mechanical): increase peristalsis against an obstructing agent. eg. gall stone, hernia
b) Adynamic: peristalsis absent, eg, paralytic ileus
D. According to the site of involvement of pathological process:
a) In the lumen
- Gallstone
- Parasites eg, round worm
- Foreign bodies eg. marbles
b) Intra-mural:
- Stricture
- Malignancy
e) Extra-mural:
- Bands/adhesions
- Hernias
- Volvulus
- Intussusception
E. Older classification: (according to complication)
a) Simple obstruction
b) Strangulated obstruction
c) Close loop obstruction: volvulus, rotation
Causes of Small Gut Obstruction:
A. Dynamic (mechanical):
a. In the lumen:
- Parasites (round worm)
- Faccolith
- Bolus of undigested food
- Foreign body
b. In the wall:
- Gall stone ileus
- Intussusceptions
- Inflammatory stricture due to: Intestinal TB, Crohn’s disease
- Carcinoma colon
- Atresia
- Diverticulitis
c. Outside the wall:
- Obstructed or strangulated hernia
- Bands and adhesion
- volvulus
- Any extra mural mass eg, enlarged lymph nodes
B. Adynamic (paralytic):
a. Paralytic ileus:
- Post operative
- Infection: peritonitis
- Metabolic:, Hypokalaemia, uraemia
- Reflux ileus: eg. Spinal injury
b. Mesenteric vascular occlusion
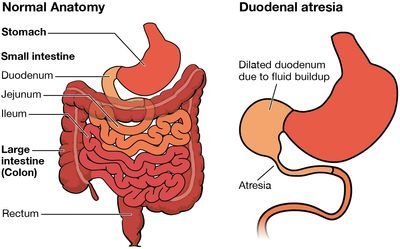
Causes of Neonatal Intestinal Obstruction:
Congenital atresia and stenosis of-
✔ Duodenum 35%
✔ Jejunum 15%
✔ lleum 25%
✔ Ascending colon 10%
✔ Multiple sites 15%
- volvulus of the mid gut (volvulus neonatorum)
- Meconium ileus
- Arrested rotation of caecum
- Imperforated anus
- Hirschprung’s disease
Management of Bowel Obstruction:
Clinical features:
A. Symptoms:
a). Pain-
- Sudden onset of abdominal pain
- Colicky pain which lasts for 3-5 min and comes after an interval of short period.
- Centrally located then spread over the whole abdomen
b) Vomiting:
- If jejunum is obstruction: may vomit once, then pain without vomiting, then again
- copious, forcible, repeated vomiting.
- Vomitus first contains undigested, then yellowish or greenish regurgitation of bile.
c) Distension:
- Early case: Slight or absent
- Late: Distension present
d) Constipation: Usually absolute constipation is a late feature
B. Sign:
a) General: Dehydration, mild anemia
b) Abdomen:
- Inspection: (a) Abdomen is distended; (b) Visible peristalsis may be present
- Palpation: (a) Generalized tenderness, (b) Carcinoma or intussusceptions
- Percussion: Hyper tympanitic
- Auscultation: Bowel sound are-
✔ At first hyperactive, loud and frequent
✔ Then resonant and high pitched
✔ Eventually tinkling
Investigation
1. Plain X-ray
2. Contrast radiograph
3. Ultrasonography scan
4. CT scan
Treatment:
a. Initially conservative treatment:
- NPO
- NG suction
- IV fluid
- Input output chart maintenance
- Antibiotics
b. Resuscitation: Fluid and electrolyte replacement
c. Surgery: (when conservative Rx fails):
Option:
- Relief of obstruction
- Division of bands and adhesions
- Untwisting of volvulus
- Resection of gangrenous part
- Repair-eg. repair of obstruction hernia
Difference between Small and Large Gut Obstruction:
| Point | Small Gut Obstruction | Large Gut Obstruction |
| Mode onset | Acute intestinal obstruction | Chronic/acute or chronic obstruction |
| Pain | Central, severe colicky abdominal pain (peril-umbilical) | Start at lower abdomen, less severe, colicky |
| Vomiting | Early and usually profuse | Late vomiting which is faeculent (smell of faeces) |
| Abdominal distension | Central, minimal, late | Peripheral, early, pronounced |
| Dehydration | Rapid and marked due to vomiting | Often absent |
| Absolute constipation | Late | Early |
| Visible peristalsis | Step ladder pattern in umbilical area | Peristalsis from right to left |
| Radiological | Shows straight segments are generally central and lie transversely. No gas is seen in the colon Jejunum volvuli conniventes | Shows haustral folds, which are spaced irregularly and the indentations is note placed opposite one another. |