Cardiovascular Disease In Pregnancy – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Cardiovascular Disease In Pregnancy
Cardiovascular changes during pregnancy:
A. Anatomical changes:
a. The heart is pushed upwards and outwards with slight rotation to left due to elevation of the diaphragm consequent to the enlarged uterus.
B. Changes in blood pressure:
In pregnancy smooth muscle relaxation occurs (due to progesterone, NO, prostaglandins or ANP)
↓
Decreased systernic peripheral vascular resistance (21%)
↓
i. blood pressure (in spite of large increases in cardiac output)
C. Changes in cardiac output:
a. Starts to increase from 5th week & reaches the peak at about 30-34 weeks.
b. It is highest in the right or left lateral or knee-chest position
c. It is lowest in supine or sitting position.
d. It increases more during labour (+50%) and immediately after delivery (+70%)
D. Causes of increase cardiac output:
a. To meet the additional O2 required due to increased metabolic activity during pregnancy.
E. Increased blood volume
Haematological changes occur during pregnancy:
Blood volume:
➤ Blood volume is markedly raised during pregnancy which starts to increase from 6ft week.
➤ Blood volume increases rapidly up to 40-5070 above the non-pregnant level at 32 weeks & remains almost static till terms.
➤ Vascularity of the uterus also increased.
RBC & haemoglobin:
➤ RBC volume is increased to 20-30%. Total increase in volume is 350 ml. Reticulocyte count increases 20%.
➤ Erythropoietin level is increased.
➤ Haemodilution:
➤ The disproportionate increase in plasma & RBC volume produces haemodilution which protects the mother from adverse effects of blood loss during delivery & diminished blood viscosity that ensures optimum gaseous exchange between the maternal & fetal circulation.
White blood cells:
Neutrophilic leukocytosis: 10000-15000/mm3 & even up to 20000 during labour.
Plasma volume:
Total plasma volume increases to the extent of 1.25 litre& greater in multiple pregnancy, multigravida & in large baby.
Total protein:
➤ Total plasma protein increases from the normal 180 gm (non-pregnant) to 230 gm at term.
➤ A:G ratio becomes 1:1 (pre-pregnant is 1.7: 1).
Blood coagulation factor:
➤Increases fibrinogen level.
➤ High ESR.
Complications of heart disease on pregnancy:
A. Maternal:
➤ Cardiac failure.
➤ Pulmonary edema.
➤ Pulmonary embolism.
➤ Active rheumatic carditis.
➤ Subacute bacterial endocarditis (SABE)
➤ Rupture of cerebral aneurism.
B. Fetal complications:
➤ Preterm labour.
➤ Intrauterine growth retardation (IUGR).
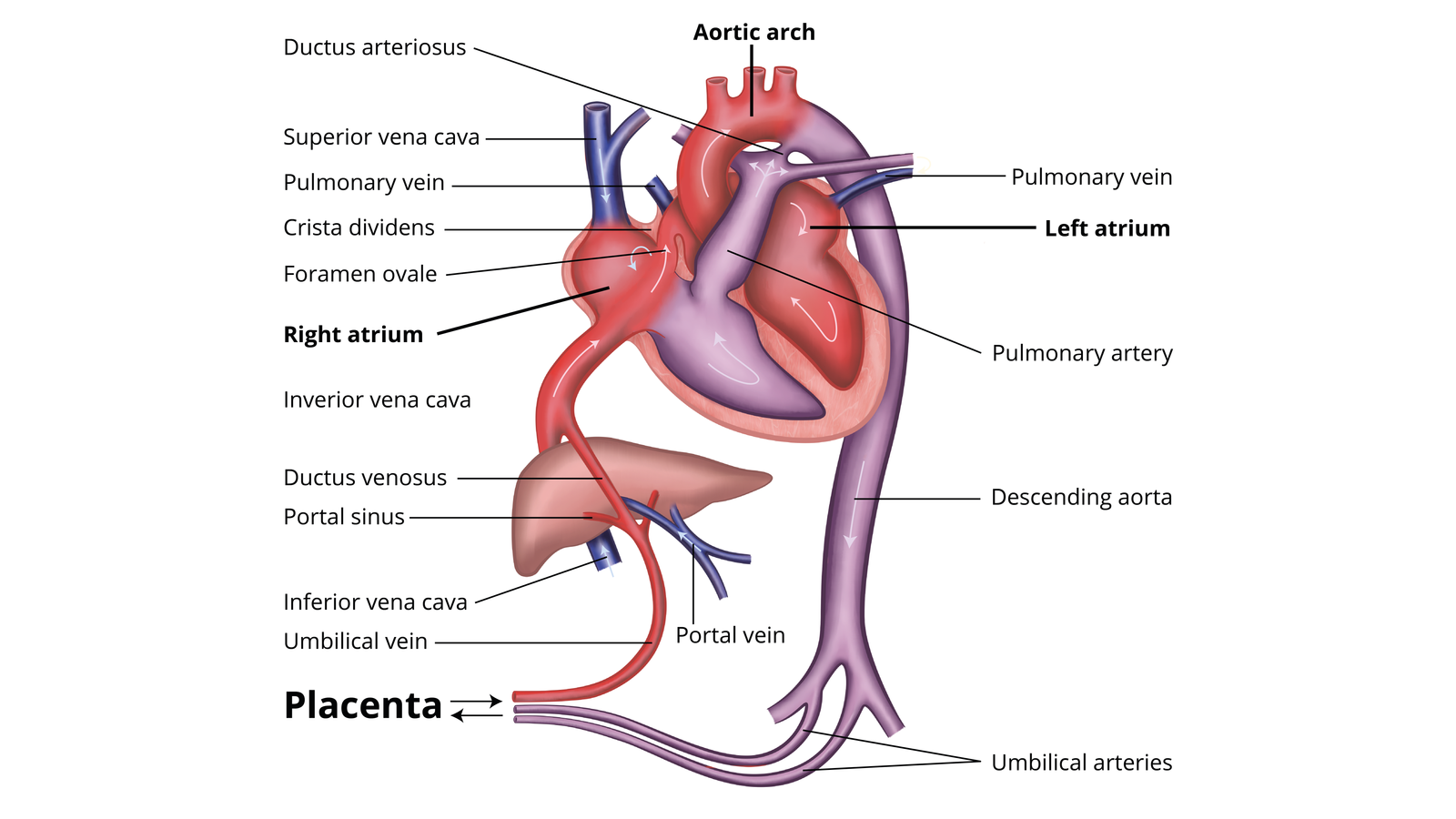
Foetal circulation:
It is special type of circulation occurs in foetus, which can be differentiated from the circulation of adult in several aspects & is essential for survive of the foetus.
Mechanism:
➤ Blood from the placenta- about 80% saturated with oxygen-passes to the foetus through the umbilical vein.
➤ On approaching the liver, the main portion of this blood flows through the ductus venosus directly into the inferior vena cava. A smaller portion enters the liver sinusoids & mixes here with the blood from the portal circulation.
➤ Blood from the inferior vena cava after reaching the right atrium, divides into two portions
larger portion of it passes through the foramen ovale to the left atrium & smaller portion
mixed here with the deoxygenated blood from the superior vena cava, which collects blood
from the upper half of the body.
➤ Blood from the left atrium passes to the left ventricle & pumped out through the aorta, mainly to the upper half of the body,
➤ The mixed blood from the right atrium passes to the right ventricle. This blood passes through the pulmonary artery to the lung & through the ductus arteriosus to the descending
thoracic aorta.
➤ Blood from the descending thoracic aorta passes to the lower half of the body, but most of it passes to the placenta via the umbilical artery for oxygenation.
Vascular changes that occur at birth:
➤ Closure of umbilical arteries.
➤ Closure of left umbilical vein.
➤ Closure of the ductus venosus. Closure of the ductus arteriosus.
➤ Closure of foramen ovale.