Carpus fracture – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Carpus fracture | CHAPTER 5 | Orthopedic Nursing
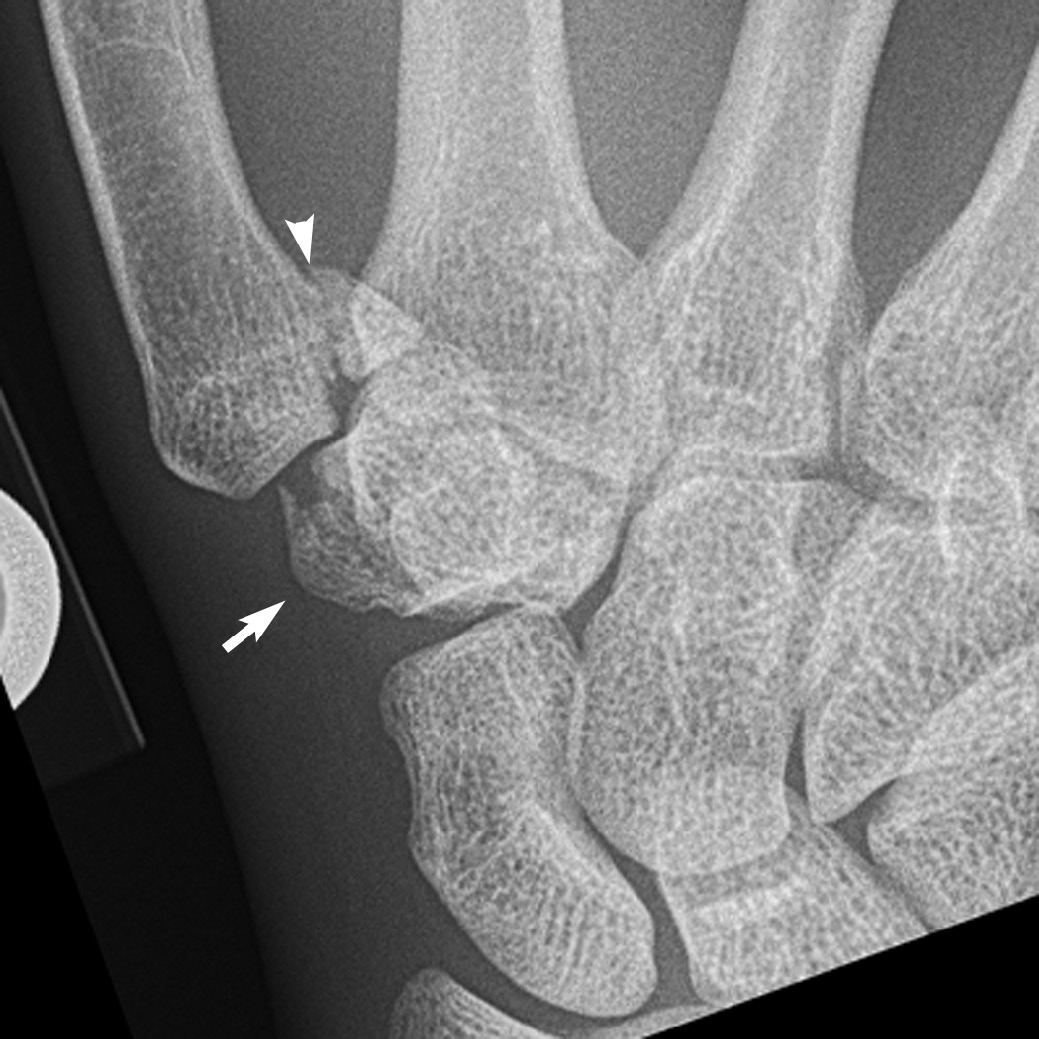
Clinical features of carpus fracture:
1. Pain.
2. Swelling.
3. Tenderness.
4. Loss of wrist movement.
5. Careful examination of the entire wrist is mandatory to localize the nature and type of injury.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-184]

Anatomical classification of scaphoid fracture:
1. Proximal pole fracture (20%).
2. Waist fracture (70%),
3. Distal body fracture (10%).
4. Tuberosity fracture,
5. Osteochondral fracture.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-185]
Management of carpus fracture:
A) Conservative methods: In case of undisplaced fracture short arm cast from proximal forearm to midpalmer area with proximal phalanx of the thumb is put.
B) Surgical methods:
1) K-wire.
2) ORIF.
Complications of scaphoid fracture:
- Delayed union.
- Non-union.
- Avascular necrosis of the proximal fragment.
- Stiffness of the wrist.
- Osteoartritic change.
- Persistent pain in the wrist.
[Ref-Dr. M.A.H.M. Jafar’s “Fracture and Dislocations” 2nd edition page-455]