
Closed Fracture- An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
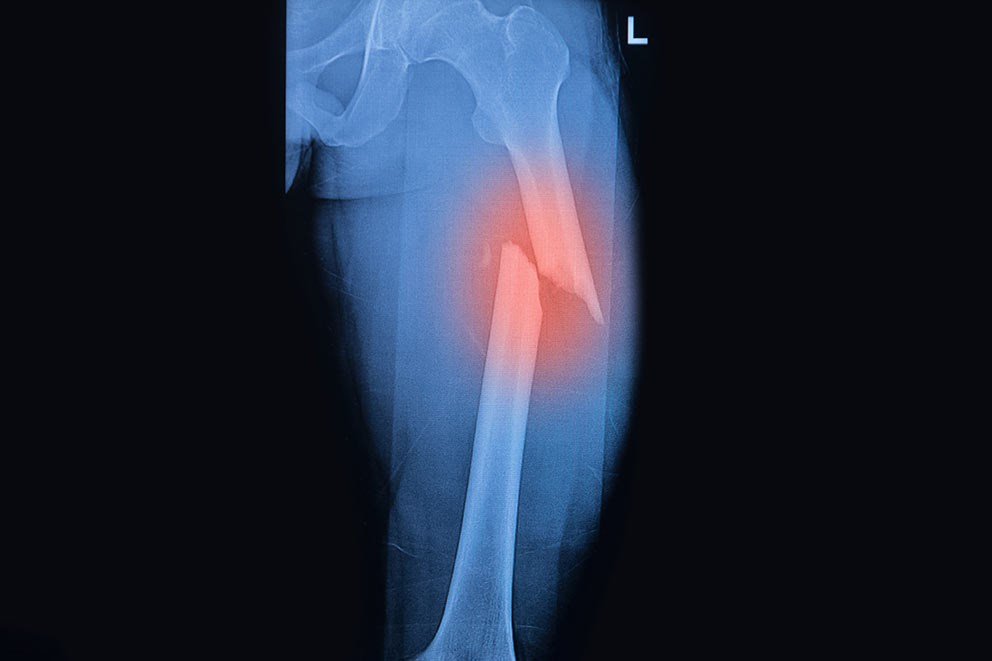
Closed Fracture
Define simple fracture:
When the fracture has no communication with the external air is called closed fracture.
Types of simple fracture:
A) According to Tschereme, 1984, closed fracture divided into the followings,
1) Grade 0: A simple fracture with little or no soft tissue injury.
2) Grade 1: a fracture with superficial abrasion or bruising of the skin and subcutaneous tissue. 3) Grade 2: a more severe fracture with deep soft tissue contusion and swelling.
4) Grade 3: a severe injury with marked soft tissue damage and a threatened compartment syndrome,
[Ref-Appleys, System of orthopedics and fracture, 9th edition,695]
B) On the basis of position of fracture fragments:
1) Undisplaced fracture:It is a condition where the fracture fragments is not displaced from its original sites.

2) Displaced fracture: Where the fracture fragments is displaced from its normal state.
How fractures are displaced :
After a complete fracture, the fragments usually become displaced by force of injury, pull of muscle gravity.
1) Translation (Shift) : The fragments may be shifted sideways, backward or forward in relation to each other.
2) Angulations (Tilt): The fragments may be angulated in relation to each other. Mal-alignment, if uncorrected may lead to deformity of the thumb.
3) Rotation (Twist): One of the fragments may be twisted on its longitudinal axis.
4) Length: The fragments may be distracted and separated or they may be overlap, due to muscle spasms causing shortening of the limb.
[Ref-Appleys, System of orthopedics and fracture, 9th edition, 689]
Medical management of a closed fracture: Simple /Closed fracture are managed by-
A) Conservative methods.
B) Operative methods.
A) Conservative methods: It depends on fracture is displaced or undisplaced.
1) For undisplaced fracture:
a) Cuff and collar sling: For upper limb fractures.
b) Strapping :For fracture of clavicle,ribs, fingers and toes.
c) Plaster slab: POP slabs can be used to support the injured limb usually as a first aid measures.
d) Rest and NSAIDs: For pain relief and reduce the inflammation.
2) For displaced fracture: here the aim is to restore back the normal anatomy of the bone either closed or open reduction.
Closed reduction is consist of 4 Rs.
a) Resuscitation resuscitation is the topmost priority if the patients in shock. And should follows
A to F managements.
- Airway,
- Breathing,
- Circulation,
- Disability,
- Exposure with environmental control,
- Fluid resuscitation.
b) Reduction: reducing the gap between displaced bone common method are
- Closed reduction: it is usually adopted for simple fracture. traction and counter traction method are known as closed reduction. It is blind technique and require skilled personnel.
- Continuous traction: Gallows traction, Balanced skeletal traction.
- Open reduction: It is done only when the above measures are fail to manage thepatients.
c) Retention:Once the fracture fragment s are reduced it hae to retained in that position till the fracture unites otherwise it tends to get displaced due to action of muscle. Retention methods after closed reduction are, POP splints, Continuous traction (Skin or skeletal traction),use of functional brace.
e) Rehabilitation: is by the way of physiotherapy and exercise (both active and passive exercise)
B) Operative method: When conservative method are failed operative methods are taken to manage the patients by open reduction using implants like,plate, screw, IM nail, Interlocking nail etc.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-21]
Open reduction technique :
Open reduction is a method in which the fracture site is surgically opened and the fracture fragments replaced into a correct anatomical position.
[Ref-Lippincott, Adult orthopedic nursing, 1 edition,page-92]
Principle of open reduction: Principles of open reduction as suggested by Lambotte includes,
1) Exposure: The fracture is adequately exposed through a proper approach.
2) Reduction: reduction or the fracture fragments under direct vision is carried out.
3) Temporary stabilization: of the fracture fragments by K-wire is done first if necessary.
4) Definitive stabilization: of the fracture using plate and screw or IM nail etc done later
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-22]
Indications of open reduction :
A) Absolute indication:
1) Failed closed reduction
2) Displaced intraarticular fracture.
3) Type III and IV epiphyseal injuries.
4) Major avulsion fracture.
5) Nonunion.
6) Replantation of extremity.
B) Relative indications:
1. Multiple fracture.
2. Delayed union.
3. Loss of reduction.
4. Pathological fracture.
5. Closed methods are ineffective in monteggia fracture, femoral neck fracture.
6. For better nursing care.
C) Questionable:
1) Neurovascular injury.
2) Open fracture..
3) Cosmetic reasons.
4) Economic consideration.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition, page-22]
Contraindication of open reduction:
2) Infection
3) Small fragments.
4) Weak and porotic bone.
5) Soft tissue damage.
6) Undisplaced or impacted fracture.
7) Poor general and medical conditions.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition,page-22]
Common fractures of upper limb :
1. Colle’s fracture.
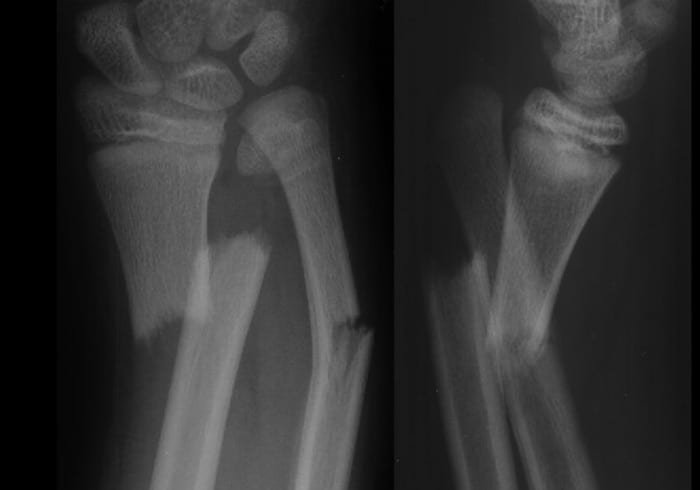
2. Fracture of shaft of radius & ulna.
3. Supracondylar fracture.
4. Fracture neck of humerus.
5. Fracture shaft of humerus.
6. Fracture clavicle.
[Ref-Dr. Jahir’ “Surgery I” Paper” 4th Edition, Page-536]