Concept about Rickets – This book covers the entire syllabus of “Nutrition and Dietetics” prescribed by BNMC-for all Diploma in Nursing Science and Midwifery students. We tried to accommodate latest information and topics.
This book is examination friendly setup according to the teachers’ lectures and examination’s questions. At the end of the book previous university questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourished. The unique way of presentation may make your reading of the book a pleasurable experience.
Concept about Rickets
Effects of vitamin -D deficiency:
Rickets:
It is a disease of young children (6 months to 2 years) characterized by:
- Growth failure
- Bone deformity
- Muscular hypotonia
- Tetany
- Convulsion due to hypocalcemia.
There is an elevated concentration of alkaline phosphatase in the serum.
Osteomalacia in adults;
- In adult vitamin D deficiency may result in osteomalacia which occurs mainly in women, especially during pregnancy and lactation when requirements of vitamin D are increase.
Definition of Rickets:
Rickets is a disorder of growing due to deficiency of vitamin D in which there is failure of mineralization of the epiphyseal growth plate, newly formed bony matrix (osteoid).
Classification:
A. Nutritional rickets:
- Lack of vitamin D
- Other factors: Decreased exposure to the sun due to dark skin pigmentation, urban living conditions and the winter season.
B. Rickets associated with abnormal metabolism of vitamin D:
- Vitamin D dependent rickets
- Chronic renal disease
- Chronic anticonvulsant therapy
- Chronic liver disease
C. Rickets due to mineral deficiency:
- Familial hypophosphatemic rickets or vitamin D resistant rickets
- Rickets of prematurity
D. Related conditions resembling rickets:
- Hypophosphatasia
- Metaphyseal dysostosis
The clinical features, investigation and management of rickets
A. Clinical features:
1. Vary with the age of onset of rickets
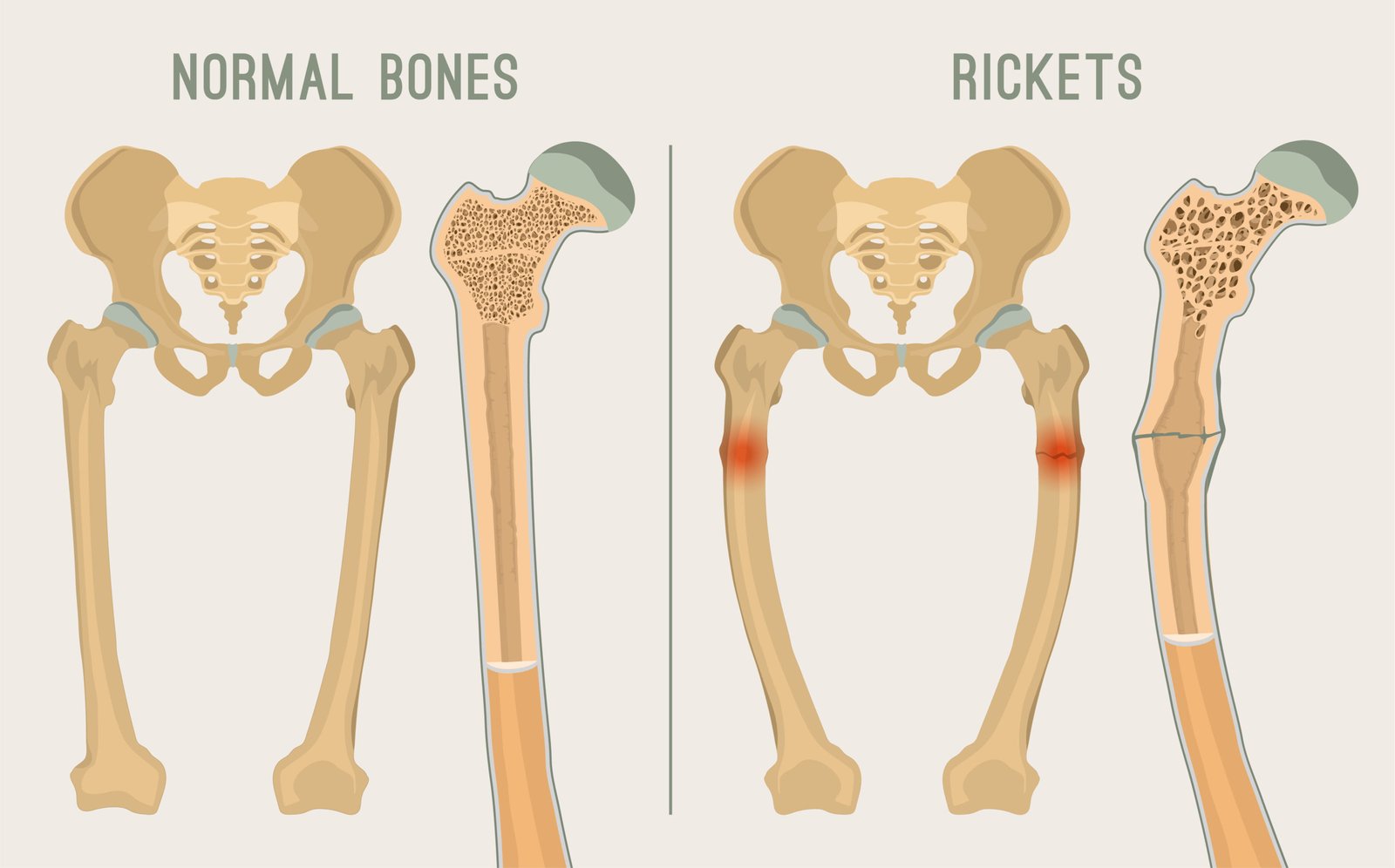
2. Skeletal deformity
- Dwarfism, frontal bossing, craniotabes, philosophers head
- Genu varum (bow leg): genu valgum (knock knee)
3. Swelling of wrist (deformity of forearm)
4. Rachitic rosary – Swelling of costochondral junction of ribs
5. Harrison’s sulcus – Depression of lower ribs along the attachment of diaphragm
6. Delayed closure of anterior fontanelle
7. Spinal deformity eg. kyphoscoliosis
8. Protuberance of abdomen, pelvic deformity
9. Hypotonia with delay in motor development
10. Tetany and convulstion
B. Investigation:
1. Calcium: Normal or decreased
2. Phosphate: Decreased
3. Alkaline phosphatase: Increased
4. Parathyroid hormone (PTH): increased
5. 1.25 (OH)2 D3: Normal or decreased
6. X-ray of knee, ankle, wrist: Cupping, fraying and widening of the distal ends of the long bone with generalized rarefaction.
C. Management:
1. Vitamin D supplementation and intake of calcium (milk)
- Vitamin D 25-125 µg (1000-5000 IU) daily for 6-8 weeks
- Stoss therapy with 3 Lac IU as a single dose for rapid healing calciferol 6 tablets at once (one tablets 50000 IU)
2. Then daily allowance of 10 µg (400 IU) daily
3. Treatment of underlying cause
4. Biochemical checkup monthly
5. If tetany develops: injection calcium gluconate
6. Surgical correction of deformity
Prevention of Vitamin D Deficiency:
- Educating parents to expose their children regularly to sunshine.
- Periodic dosing (prophylaxis) of young children with vitamin D; and
- Fortification of foods, especially milk.

Scurvy
Clinical Manifestations of Scurvy in Infants and Young Children:
Most frequent symptoms
- General irritability
- Tenderness of the limbs, especially of the legs
- Pseudo paralysis, usually involving the lower extremities
- Involvement of costochondral junctions: changes such as beading of ribs
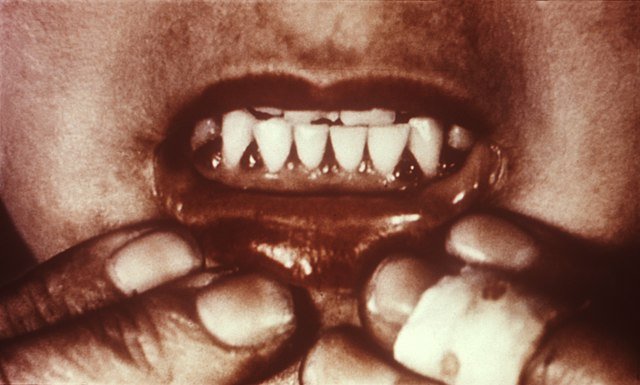
- Haemorrhage around erupting teeth (in infants without teeth gums appear normal)
- Anaemia
Possible symptoms:
- Anorexia
- Low-grade fever
- Mild diarrhoea, sometimes bloody
- Petechial haemorrhages in the skin
Prevention of Scurvy/Vitamin C Deficiency in Children:
The main approaches to preventing the onset of scurvy in emergency situations affecting large populations are as follows:
1. Providing food rations containing adequate amounts of vitamin C by increasing the variety of the food basket and regularly including fresh fruit and vegetables.
2. Providing sufficient food in the ration to allow refugees to sell the surplus for other purposes.
3. It has been found that refugees with the highest value of rations received did, in fact, consume the greatest amounts of fruit and vegetables (Hansch, 1992).
4. Fortifying current relief commodities with vitamin C, e.g. providing fortified blended cereallegume food in the general ration in sufficient amounts to cover vitamin C requirements.
5. Providing vitamin C supplements in the form of tablets at least weekly,
6. Encouraging and facilitating, where feasible, cultivation by refugees of fruits and vegetables in home gardens