Concept about Tubectomy- This book covers the entire syllabus of “Community Health Nursing” prescribed by the Universities of Bangladesh- for Basic and diploma nursing students. We tried to accommodate latest information and topics.
This book is examination friendly setup according to the teachers’ lectures and examination’s questions. At the end of the book previous university questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourished. The unique way of presentation may make your reading of the book a pleasurable experience.
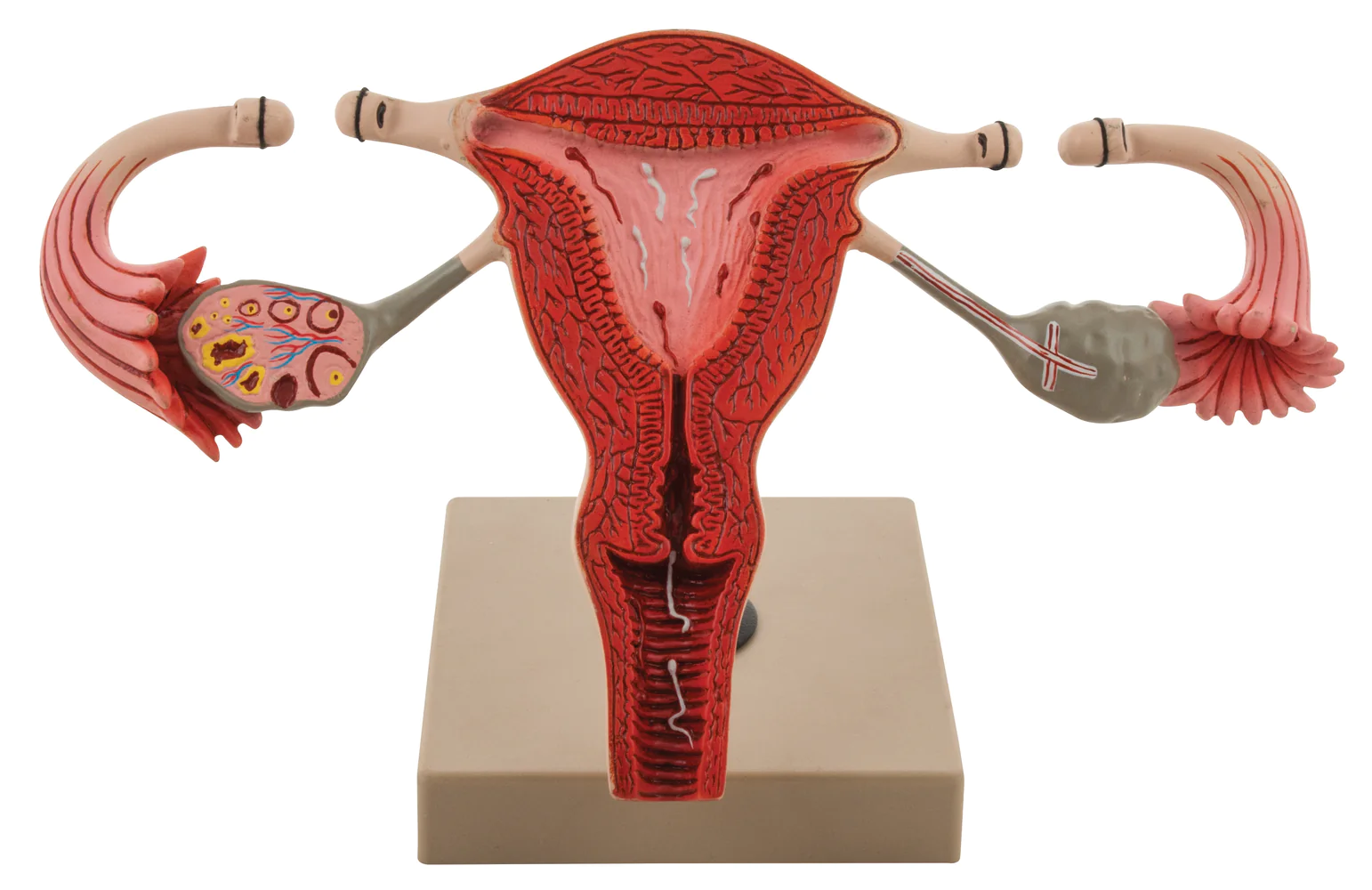
Concept about Tubectomy
Ligation of fallopian tube is a permanent contraceptive method for female.
Or
Occlusion by segment of both the fallopian tubes is called tubectomy. It is the permanent sterilization procedures for the female. Occlusion of the fallopian tubes in some form is the underlying principle to achieve female sterilization.
Advantage
1. Permanent
2. Highly effective
3. Cost effective when cost is spread out over time
4. Nothing to buy or remember
5. No significant long term side effects
6. Partner compliance not required
7. No interruption in lovemaking
Disadvantage
1. Procedures technically difficult
2. Expensive at the time performed
3. Requires surgeon, operating room, Technical assistant, medication, surgical equipment.
4. If failure, high probability of ectopic pregnancy
5. No protection against STD.
6. May cause psychological problems
7. Requires hospitalization
Complication
If client selection is appropriate and the procedure is perfect then the complications will be minimum.
A. Immediate:
- Injury of the bladder and the intestine.
- Bleeding from the mesosalphinx.
- Rectus haematoma,
- Infection of the wound or the pelvic cavity.
B. Late:
- Incisional hernia.
- Post-tubal ligation syndrome such as chronic pelvic pain and menstrual distrubances.
- Ectopic pregnancy.
- Failure of tubectomy leading to pregnancy.
Indications
1. To limit the size of the family.
2. For the purpose of population control.
3. In certain medical diseases where further pregnancy will be hazardous for the maternal health.
Preparation of a Patient for Tubal Ligation
A. Counseling:
- The patient and her husband should be informed beforehand that the method is permanent and usually is not reversible.
- The couple should be informed that it would not interfere with the conjugal life or normal household work.
- The risk of tubectomy must also be explained to the patient.
- Informed consent should be taken from the acceptors.
B. Pre-requisite:
- Detailed history regarding menstrual cycle, LMP, no. of living children, age of the last child should be taken and also history of PID, pelvic surgery, any medical diseases should be taken.
- G/E is to be done to note the pulse, BP, heart & lung condition, absence of anaemia & jaundice. Pelvic exam, is to be done to see the size, shape, position and mobility of the uterus & fornices for any pathology.
- Hb% should be estimated and must be more than 10 gm%.
- Urine analysis is to be done.
- She should be in empty stomach at least for 6 hours prior to tubectomy.
C. Pre-operative preparation:
- Half an hour before tubectomy 10 mg diazepam is given.
- Then she should void urine and is taken to the operation table.
- IV is started.
- Inj. Pethidine 50 mg, Inj. Phenergan 25 mg and Inj. Atropine 0.6 mg is given IV. The abdomen is cleaned with
- providone iodine and then drapping is done. 6.
- 1% lignocane is used
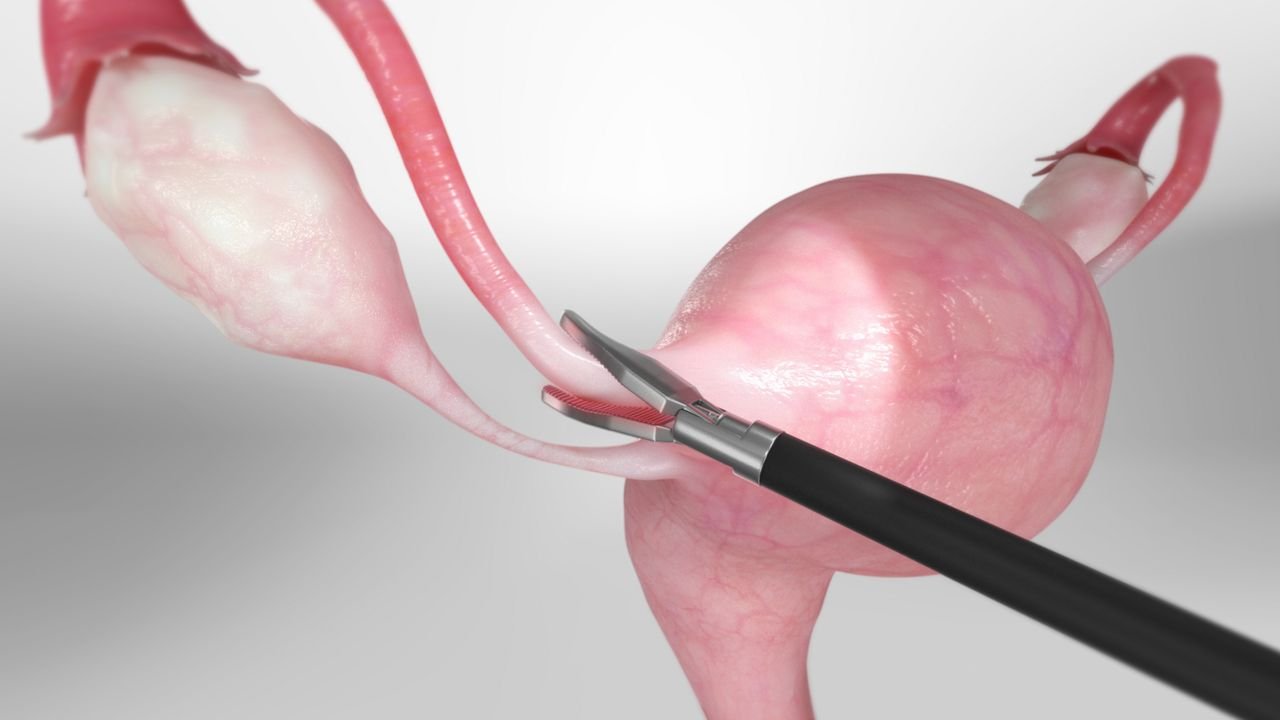
Procedure of Tubectomy
1. 1% lignocaine is used as a local anaesthetic, about 20 ml is taken is a syringe. 3-5 ml is injected under the skin at the incision site, Skin incision is given 3 minutes after the injection.
2. In interval tubectomy, a transverse incision of about 2.5 to 3 cm is made 2.5-3 cm above the symphysis pubis. The skin and subcutaneous tissue are then incised with a scalpel.
3. Another 3-5 ml of 1% lignocaine is then injected into the rectus sheath. The rectus sheath is then retracted laterally.
4. The rectus muscles are then retracted laterally.
5. 3-5 ml of lignocaine is now injected to the peritoneum that is then picked up with a pair of artery forceps, great care should be taken to avoid injury to the intestine and the bladder. The peritoneum is now incised longitudinally.
6. Small Morris retractor can be used to retract the lower margin of the wound. Five ml of 1% lignocaine is then poured over the uterus and the tubes.
7. Two fingers are introduced into the pelvic cavity and the fallopian tube is forked out through the wound seeing the fimbriae identifies the tube. It is hold with Babcock’s at the junction of the medial 1/3 rd and the lateral 2/3rd and a loop is made. The base of the loop is tied by chromic catgut followed by the excision of the knuckle of the tube and then the tube is returned to the cavity after ensuring haemostasis. Same procedure is repeated on the opposite side.