Concept Of Labour – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Concept Of Labour
Definition of Full Term Pregnancy:
When the duration of pregnancy continues up to 37 completed weeks from first day of last menstrual period the pregnancy is termed as full term pregnancy.
Definition of Labor:
Series of events take place in the genital organs of a pregnant lady in an effort to expel the viable product of conception from the womb to the exterior through vagina is called labour.
Or
The physiological process by which the fetus (viable) is expelled from the uterus into the vagina and then to the outside of the body.
Initiation of labor:
Labor is a phenomenon that depends on complicated interaction between the fetus and mother. Factors believed to be influential in the onset of labor are genetic control, myometrial stretch, increased estrogen levels, progesterone withdrawal, oxytocin sensitivy, prostaglandins and fetal and membrane factors.
Physiological changes during labor:
1. Reproductive change: uterine, cervix, changes of amniotic fluid.
2. Nervous system change
3. Cardiovascular system change
4. Fluid and electrolyte system change
5. Respiratory system change
6. Urinary system change
7. GI system change
8. Immune system change.
Factors related to labor:
There are five factors related to labor:
1. Passenger: fetus & placenta, size of the fetus, head, shoulders and position of fetus.
2. Passaway: The kind of mothers pelvis, diameter of exit there is.
3. Power: Strength of contraction and how much the mom pushes.
4. Position: best position for the mother to push.
5. Psychologic response:
a. 1st stage euphoria leads to seriousness.
b. 2nd stage: amnesia
e. 3rd stage: elation or fatigue
Or (Another answer)
There are five factors related to labor:
1. Passenger: The passage of the fetus through the birth canal is influenced by the size of the fetal head and shoulder, the dimensions of the pelvic girdle, and the fetal presentation
and position.
➤ Fetal head
➤ Shoulders and pelvic girdle
➤ Fetal lie
➤ Presentation
➤ Attitude
➤ position
2. The passageway/Passage:
➤ Pelvis
➤ Soft tissues
3. Power:
➤ Uterine contractions
➤ Voluntary bearing-down efforts
➤ Implications of nursing care
4. Psychological factors:
➤ 1st stage-euphoria leads to seriousness.
➤ 2nd stage: amnesia
➤ 3rd stage: elation or fatigue.
5. Position of the mother:
Position is the relationship of the fetal reference point (e.g., occiput, brow, chin or mentum, or sacrum) to one of the four quadrants of the mother’s pelvis; that is the most prominent and dependent portion of the presenting part is related to one of the four quadrants of the moth’s pelvis.
Definition of Normal Labour:
Normal labour is one which fulfils the following criteria:
➤ The labour is started spontaneously at term (37-42 completed weeks).
➤ Foetus is vertex presentation.
➤ Without undue prolongation.
➤ Natural termination without any aid or with minimal aid (episiotomy).
➤ Without any complication affecting the health of the mother and or the baby.
Or
Normal labour is the physiological process of spontaneous uncomplicated and not delayed expulsion per vaginal of mature fetus with vertex presenting following by after births of umbilical cord, placenta and membranes.
Or
WHO definition of normal labour
“Spontaneous in onset, low-risk at the start of labour and remaining so throughout labour and delivery. The infant is born spontaneously in the vertex position between 37 and 42 completed weeks of pregnancy. After birth, mother and infant are in good condition.”
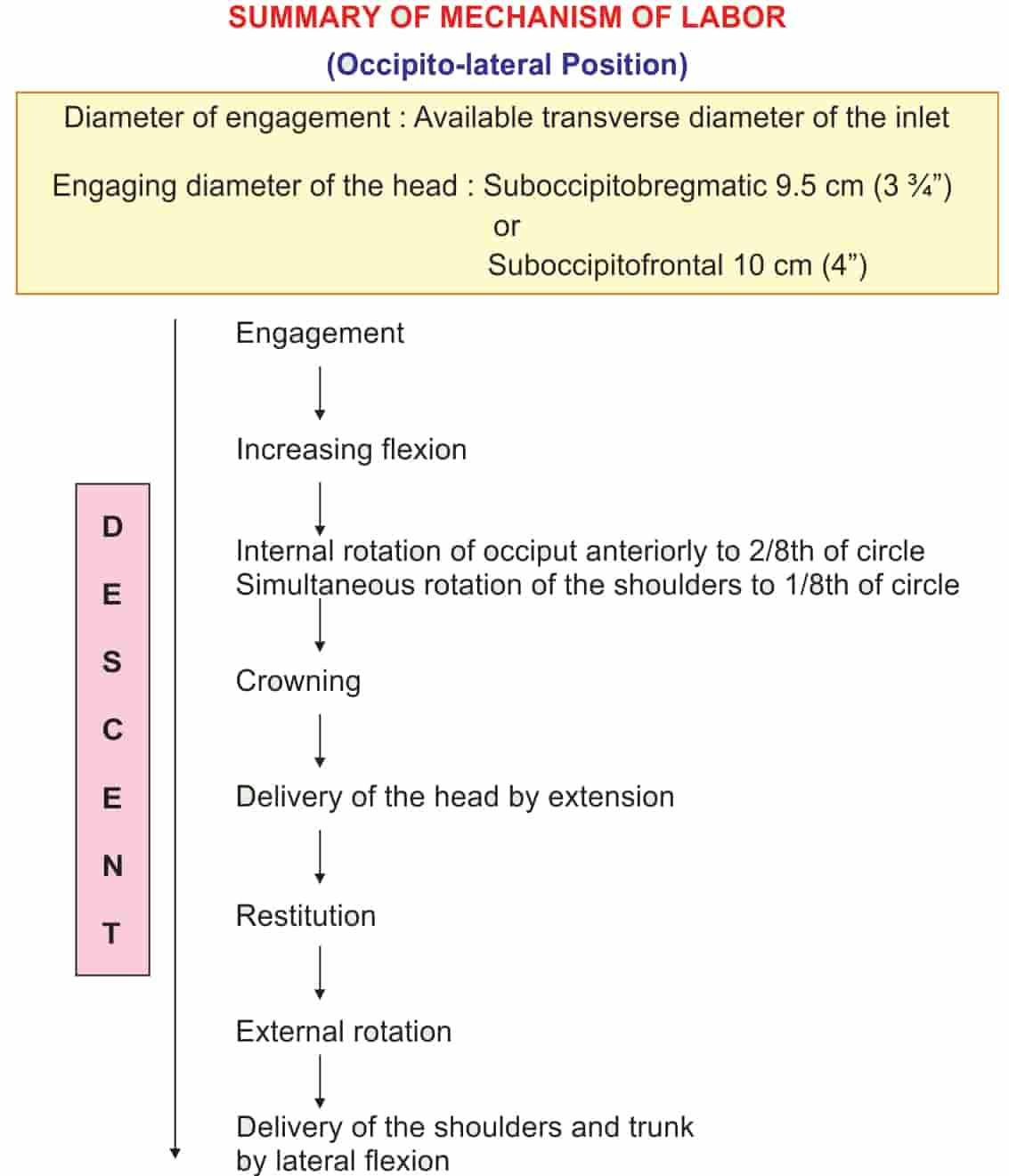
Component of Labour:
1. Head engagement
2. Descent of the head
3. Flexion of the head
4. Internal rotation
5. Crowing
6. Extension
7. Restitution
8. External rotation
9. Birth of the shoulder and trunk.
Mechanism of Normal Labour:
Mechanism of labour in short-
Diameter of engagement: Available transverse diameter of the inlet. Engaging diameter of the head: Suboccipito-bregmatic 9.5 cm (3. 3/4″) or suboccipito-frontal 10cm (4″)
Factors affecting responses to pain in labor
Factors influencing how to feel about labour pain:
1. Society’s attitudes
2. Cultural and religious beliefs
3. Birth stories
4. Fears and concerns
5. Expectations
6. Progress in labour
7. Exhaustion
8. Complications arising
9. Pain relief not meeting expectations
10. The caregiver’s influence
Equipment’s for normal delivery
A. For mother-
Sterile delivery pack containing
1. Articles for cutting and suturing an episiotomy
a. Episiotomy scissors
b. Artery clamps – 3
c. Tissue forceps – 1
d. Needle holder – 1 -1
e. Syringe and needle for infiltration-10 ml
2. Scissors for cutting the cord
3. Bowl for cleaning solution
4. Basin to receive placenta
5. Cotton balls
6. Gauze pieces
7. Towel to cover the hand supporting the perineum
8. Sterile gown
9. Leggings for mother
10. Apron, gloves and mask for staff
B. For new born –
1. Baby blanket or flannel cloths-2.
One to receive and dry the baby of excess secretion and another to wrap the
baby.
2. Neonatal resuscitation equipment
3. Oxygen cylinder with tubing
4. Suction apparatus and mucous extraction
5. Cord clamps
6. Bulb syringe for nasal oropharyngeal suctioning of the baby
C. Other articles-
1. Antiseptic lotion – savlon or Dettol
2. Suture material
3. Perineal pads for mother
4. Sterile gloves
5. Methergin
6. Lignocaine 2%
Definition of passage:
The passage is refers to the route the foetus must travel from the uterus through the cervix and vagina to the external perineum. The organs are contained inside the pelvis, the fetus must pass through the pelvis ring.
Definition of passengers:
The fetus is the passengers. The body part of the fetus has the widest diameter is the head. So this part likely to be able to pass through the pelvic brim. When a fetal skull can pass depends on both its structures (bones, fontanels and sutures) and its alignment with the pelvis.
Definition of attitude
The Relationship of the different parts of the fetus to each other. Relationship of fetal head to
spine:
➤ flexed, (this is the normal situation)
➤ neutral (“military”),
➤ extended.
➤ hyperextended
Definition of engagement:
It means the maximum diameter of the presenting part has passed the pelvic brim. When the greatest horizontal diameter has passed the plane of pelvic brim, the head is said to be engaged. In primigravida engagement usually occurs before the onset of labor and in multiparae it occurs in late first stage.
Time of engagement:
b. In Primigravidae: Usually before the onset of labor.
c. Usually in late first stage of labor
Definition of station:
The relation of the presenting part of the fetus to the level of the ischial spines. It is called “0” station. If the presenting part is above the spines, the distance is measured and described as minus station, which range from (-1 cm to 4 cm). When the presenting is below the ischial spines, the distance is stated as plus station (+1 cm to + 4cm) At a +3 or + 4 station, the presenting part at the perineum and can be seen the vulva is separated with crowning.
Definition of Lie
Lie indicates the relation with the long axis of the foetus bears to that of the mother. Whenever the fetus is lying in a horizontal (transverse) or vertical (longitudinal) position.
Relationship between the longitudinal axis of fetus and mother:
➤ longitudinal, (resulting in either cephalic or breech presentation)
➤ oskie, (cephalic presentation, fetus legs straight along frontal axis of mother)
➤ oblique, (unstable, will eventually become either transverse or longitudinal)
➤ transverse (resulting in shoulder presentation)
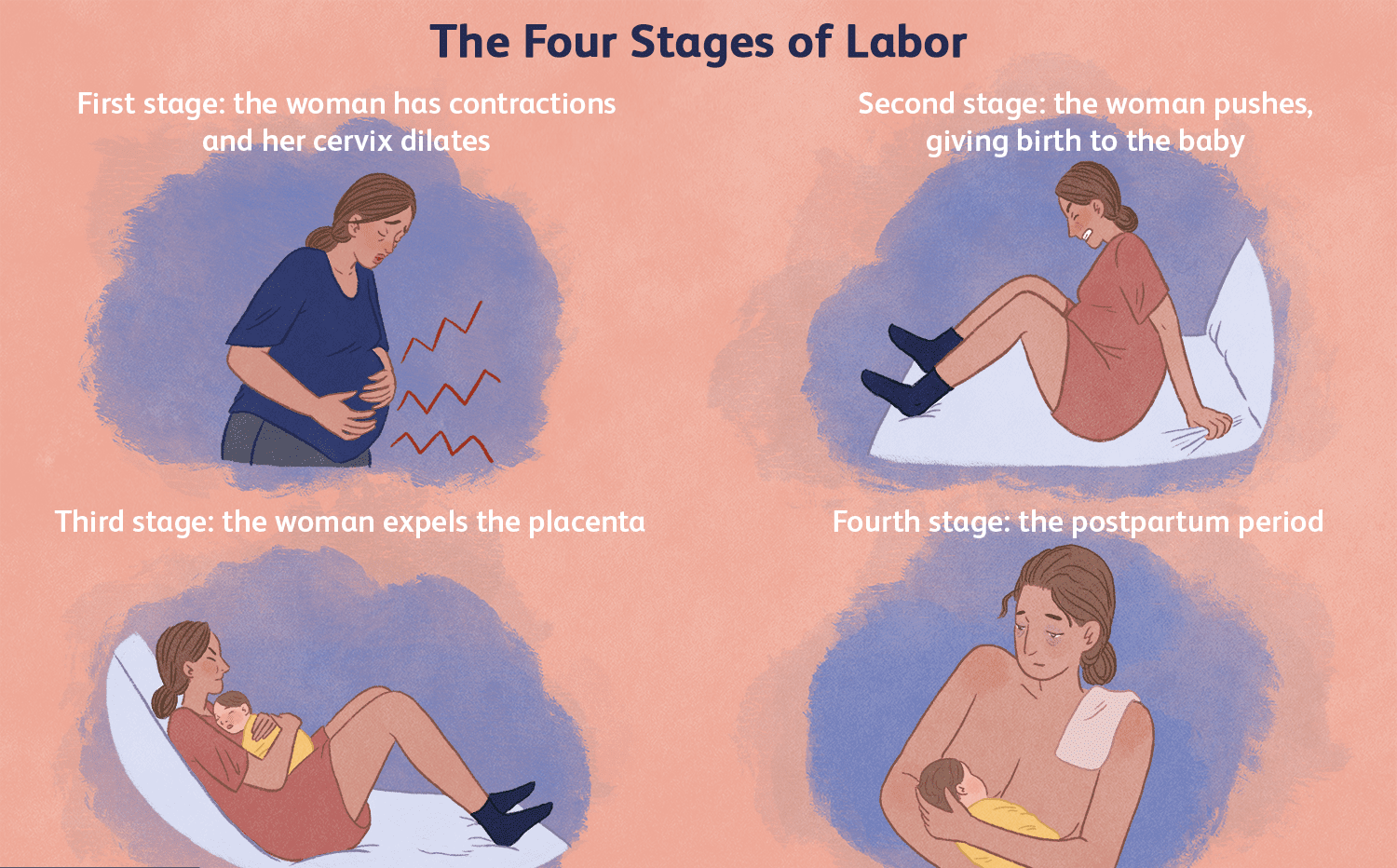
Stages of Labour:
1. First stage: From the onset of true labour pain to full dilatation of the cervix (10 cm).
| Primigravidae | 12 hours |
| Multiparae | 6 hours |
2. Second stage: From full dilatation of the cervix (10 cm) to complete expulsion of the fetus.
| Primigravidae | 2 hours |
| Multiparae | 30 minutes |
3. Third stages: From complete expulsion of the fetus to complete expulsion of the placenta.
| Primigravidae | 15-30 minutes |
| Multiparae | 15 minutes |
4. Fourth stage: It is the stages of observation for at least one hour after expulsion after births. During this period, general condition of the patient and the behavior of the uterus are to be carefully watched.

Phases of labor:
A. Phase 1: carly (latent) labor:
The first of the three stages of labor is usually the longest, but thankfully it’s also the least intense, by far. During early labor, following labor signs appear:
➤ Backache (constant or with each contraction)
➤ Menstrual-like cramps
➤ Lower abdominal pressure
➤ Indigestion
➤ Diarrhea
➤ A sensation of warmth in the abdomen
➤ Blood-tinged mucous discharge.
➤ Rupture of the amniotic membranes.
B. Phase 2: active labor:
The active phase of labor usually lasts from two to three-and-a-half hours (with a wide range of what’s considered normal) as cervix dilates to 7 centimeters.
During active phase of labor, following labor signs appear:
➤ Increasing pain and discomfort with contractions
➤Increasing backache
➤ Leg discomfort or heaviness.
➤ Fatigue.
➤ Increasing bloody show.
➤ Rupture of the membranes.
C. Phase 3: transitional (advanced) labor:
During transitional labor the last, most intensive phase of labor, cervix will dilate from 7 to its final 10 centimeters. Fortunately it’s also the shortest, generally lasting from 15 minutes to an hour (though it can sometimes take up to three hours).
During transitional labor, following labor signs appear:
➤ Strong pressure in the lower back and/or perineum,
➤ Rectal pressure, with or without an urge to push.
➤ An increase in bloody show as capillaries in the cervix rupture.
➤ Feeling very warm and sweaty or chilled and shaky.
➤ Crampy legs that may tremble uncontrollably.
➤ Nausea and/or vomiting.
➤ Drowsiness between contractions.
➤ A tightening sensation in your throat or chest.
➤ Fatigue or exhaustion.
Definition of Latent phase of labour
The early stage of labor that is characterized by irregular, infrequent, and mild contractions and little or no dilation of thecervix or descent of the fetus.
Or
The latent phase of labour is the time when changes in the body start occurring in preparation for actual or established labour. The latent phase is difficult to describe as it varies widely amongst individuals in terms of character and duration. However, it is generally described as a period of time, not necessarily continuous, where there are painful contractions accompanied by thinning and opening of the cervix up to 4cm.
Or
In the latent phase, contractions occur more often, become stronger, and become more regular. During this phase the cervix thins. This is called effacement. The latent phase varies from woman to woman and from labor to labor. It may take as a few hours. The latent phase tends to be 10 to 12 hours. Membranes may rupture in the early- to mid-portion of the first stage of labor. If they rupture, the labor process often speeds up.
Characteristics of latent phase
➤ It starts from onset of labour until the cervix reaches 3 cm dilatation.
➤ Once 3 cm dilatation is reached, labour enters the active phase.
➤ Lasts 8 hours or less.
➤ Each contraction lasting>20 seconds.
➤ At least 2/10 min contractions.
➤ A sensation of warmth in the abdomen.
➤ Blood-tinged mucous discharge.
➤ Rupture of the amniotic membranes.
Importance of latent phase
1. During this phase the cervix thins. This is called effacement.
2. The latent phase varies from woman to woman and from labor to labor. It may take a few days or be as short as a few hours.
3. There is some cervical change, including cervical effacement and dilatation up to 4cm.
4. The latent phase tends to be 10 to 12 hours for a woman who has had children. For first pregnancies, it may last closer to 20 hours.
5. Many women confuse the latent phase of labor with Braxton Hicks contractions.
6. Membranes may rupture in the early to mid-portion of the first stage of labor. If they rupture, the labor process often speeds up.
In the latent phase of labour, the womb begins to contract irregularly as it starts to co-ordinate the action of its muscle fibres and slowly adjusts its shape so that the cervix moves into the right position for birth. As time goes on, the contractions act upon the cervix itself, causing it to soften, thin, become stretchy and start to open.
This length of this phase can range from six hours to two-three days. Nobody knows for sure why there are such big differences in duration between individuals. It tends to be longer in the first pregnancy.
Active phase of labor
During this phase, the cervix dilates rapidly. For most women, dilation goes from 3 to 4 centimeters to 8 to 9 centimeters. The active phase is the most predictable, lasting an average of 5 hours in first-time mothers and 2 hours in mothers who have given birth before.
Characteristics of active phase
➤ Contractions at least 3/10 min
➤ Each lasting > 40 sceonds
➤ The cervix should dilate at a rate of 1 cm/hour or faster Increasing pain and discomfort with contractions
➤ Increasing bloody show.
➤ Rupture of the membranes.
➤ Leg discomfort or heaviness.
Common Labor Signs and symptoms
Although every pregnancy is different and there is no definite set of events, some common, early labor signs include:
1. Lightening: Women can breathe again! This is an indication that the baby has dropped, settling deeper into the pelvis and relieving some of the pressure on diaphragm helping women to not be so short of breath.
2. Bloody Show: Loss of mucus plug/Bloody vaginal discharge
3. Rupture of Membranes/Water Breaking
4. Early Strong and regular contractions
5. Nesting: Spurt of energy.
6. Effacement: Thinning of the cervix. In the last month of pregnancy the cervix will begin to stretch and thin.
7. Dilation: Opening of the cervix. Dilation is the process of the cervix opening in preparation for childbirth.
8. Lower back pain and cramping
9. Nausea present
10. Abdomen looks lower and more protruding.
11. Diarrhea or flu -like symptoms.
12. Braxton-Hicks contractions (false contractions) during the last week of pregnancy.
13. Frequent urinating.
Monitoring maternal well-being in labour:
A. Monitoring the maternal well-being in Labour by assessment of –
1. Temperature / Monitor the maternal temperature
a. On admission
b. Intact membranes – 4 hourly.
c. Ruptured membranes – 2 hourly.
Pyrexia may be caused by infection or ketosis and can be associated with epidural analgesia (neuraxial block)
2. Monitor the maternal pulse
a. On admission
b. During the latent phase of labour – 4 hourly
c. During the Active phase of labour – every 3 min
Tachycardia may indicate anxiety, pain, infection, Ketosis & hemorrhage.
3. Monitory /Measure the maternal BP (Blood Presser)
a. On admission
b. During latent phase of labour-4 hourly
c. During active phase of labour -2 hourly
4. Pre-eclampsia and eclampsia is coursed by high blood pressure. Monitor the maternal respiration.
5. Monitor the urine output
6. Monitor the urine test for albuminuria proteinuria.
7. Monitor the maternal general condition.
If the any abnormal condition is shown, inform the senior person..
B. Monitoring the fetal well-being in labour :
Monitoring the fetal well-being in labour by assessment of
1. Auscultate the Fetal Heart Rate (FHR) during normal Labour
a. On admission
b. Laten phase of Labour -2 hourly
c. Active phase of labour 30 minutely
2. There are four characteristics when listening to fetal heart
a. Rate- The normal fetal heart rate is between 120 to 160 beats per minute or 110 to 180 beat.
b. Variability-Changes in heart beat from baseline 5 to 25 beats.
c. Acceleration- An increase in the heart rate for longer Than 15 seconds.
d. Deceleration – A decrease in the fetal heart rate of 40 or more beats from the baseline.
3. Monitor the amniotic fluid: Women with ruptured membranes should have the amniotic fluid loss checked for colour, consistency and odor:
a. On admission.
b. In Early labour – 2 hourly
c. In active labour every 30 minutes.
Increased gastrointestinal motility resulting in meconium being passed into the amniotic fluid.Go The presence of meconium may not lead to meconium aspiration syndrome (MAS), but the fetus will require continuous heart rate monitoring during Labour. It may indicate chorioamnionitis.
Types of Labour Pain:
A. True labour pain
B. False labour pain
Tue labour pain which following features:
➤ Painful uterine contraction (labour pain) at regular intervals.
➤ The pain gradually increasing in intensity.
➤ Gradually the duration of pain is increasing.
➤ Frequency of the pain is increase.
➤ Progressive effacement and dilatation of cervix.
➤ Associated with show
➤ Formation of bag of waters.
➤ No relieved by sedatives.
It is an intermittent progressive pain gradually increasing in intensity, duration and frequency which coincides with uterine contractions.
False labour pain: It has got the following features – Dull in nature.
➤ Usually confined to the lower abdomen and groin.
➤ Continuous and unrelated with hardening of the uterus.
➤ Without any effect on dilatation of the cervix.
➤ Usually relieved by enema and administration of a sedative.
False pains are probably due to stretching of the cervix and lower uterine segment with consequent irritation of the neighboring ganglia.
Difference True and False Labour Pain:
| Points | True labour pain | False labour pain |
| 1. Onset of pain | At the onset of labour | Usually prior to onset of labour pain by 1 or 2 weeks in primi, few days in multi. |
| 2. Character | Colicky | Dull |
| 3. Nature | Sever | Dull |
| 4. Site | Back and in front of the abdomen. | Lower abdomen and groin. |
| 5. Radiation | Towards thigh | Localized |
| 6. Duration | intermittent | Persistent |
| 7. progression | Intensity increases and interval decreases gradually | Non-progressive. |
| 8. Relieving factors | Nothing | Absent |
| 9. Cervical dilatation | Present | Absent |
| 10. Show | Present | Absent |
| 11. Causes | Vigorous uterine contraction → anoxia to uterine muscle→ Ischemic pain. | Stretching of the cervix and lower uterine segment. |
Most effective positions of labor
1. During 1 stage of labour-
A. Upright position
B. Recumbent position
D. Advantages of upright position
➤ The fetus into the lower pole of the uterus & by pressing on the cervical nerve ending stimulates good uterine action.
➤ In the erect position the antero-posterior diameter of the pelvic brim is enlarged.
➤Standing on tip-toe during a contraction with women back bent & her abdominal muscles drawn inwards & upward.
➤ It helps to use gravity effectively.
E. Advantages of recumbent position
➤ The women should of course be in bed So that she can relax & conserve her strength.
2. During 2nd stage of labour
A. Squating position
B. Lying on side position
C. Kneeling position (on hands or fore arms and knees)
A. Advantages of squating position
➤ It uses gravity to help baby’s descent.
➤It can help to open the pelvis
B. Advantages of lying on side position
➤ It help to prevent tears
➤ It promotes rest and relaxation between pushing and contractions.
C. Advantages of lying on side position
➤ It helps to encourage movement of the baby.
➤ The women can drape over the head of the bed, or birthing ball, to rest and relax.
➤ It may relieve back pain during labour.
➤ It helps baby rotates to most favorable position.
3. During 3rd stage of labour
A. Dorsal position.
Advantages of this position
➤The uterus can be observed better.
➤ It assist to expel the placenta
➤ It helps to reduce risk of air embolism.

Progressive of labour can be assessed by the following ways:
a) Uterine contraction: It gradually increases in intensity, frequency and duration which are assessed by per abdominal palpation.
➤ 3 times per 10 minutes
➤ Each contraction lasts for 40-60 second.
➤ Strong enough
b) Dilatation of cervix:
➤ Dilation of cervix (in cm)
➤ Effacement of cervix (in %)
➤ Consistency and position of cervix
➤ Presence or absence of fore waters
➤ State of liquor if any
➤ Status of membranes
c) Descent of foetal head/presenting part:
✔Per abdominal examination:
The descent of foetal head is assessed from level of the head in relation to the brim of pelvis and is measured in fifths. The width of the 5 fingers is a guide to the expression in fifths of the head above the brim-
5/5-Head floating above the brim-
➤ 4/5-Fixing
➤ 3/5-Not engaged
➤ 2/5-Just engaged
➤ 1/5- Engaged
➤ 0/5-Deeply engaged
Per-vaginal examination:
➤ Descent is judged by zero station – rotation of the head with ischial spine. Zero is the level of the ischial spine, i.e. mid pelvis and estimation are in cm above zero.
➤ Postion of occiput can be felt.
➤ Caput and moulding can also be felt.
✔ Auscultation of foetal heart sound: Shifting of FHS downwards towards the pubic symphysis.
Ten common labor complications:
1. Failure to progress
2. Fetal distress
3. Perinatal asphyxia
4. Shoulder dystocia
5. Excessive bleeding
6. Malposition
7. Placenta previa
8. Cephalopelvic disproportion
9. Uterine rupture
10. Rapid labor.