Concept of Peptic Ulcer Disease (PUD) – This book covers the entire syllabus of “Pharmacology” prescribed by BNMC- for diploma in nursing science & midwifery students. We tried to accommodate the latest information and topics. This book is an examination setup according to the teachers’ lectures and examination questions.
At the end of the book, previous questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourish. The unique way of presentation may make your reading of the book a pleasurable experience.
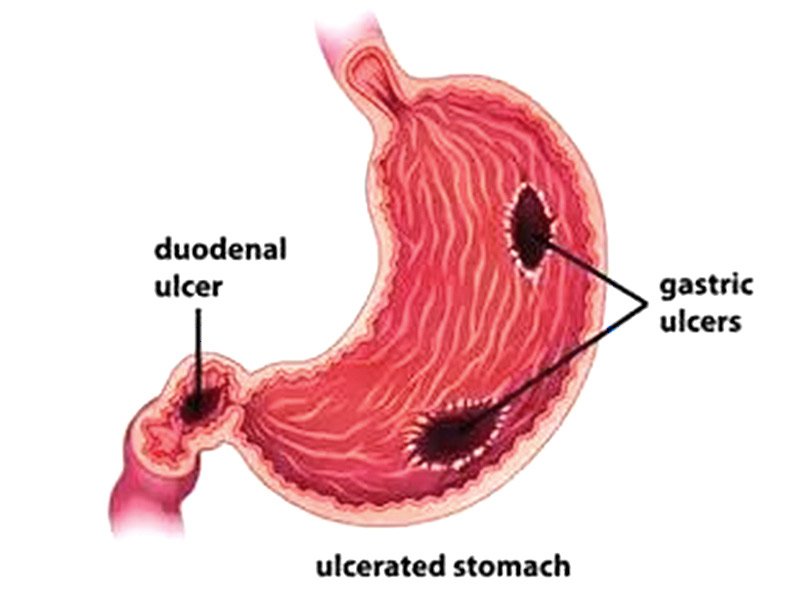
Concept of Peptic Ulcer Disease (PUD)
Ulceration in the gastric mucosa due to acid-pepsin digestion is called peptic ulcer disease peptic ulceration is caused by an imbalance between:
- Acid and pepsin, and
- Mucosal defense: Mucus, bicarbonate and prostaglandin.
- Helicobactor pylori (urease-producing bacterium found in the stomach)
Approaches of treatment of PUD
There are four main approaches of treatment:
1. Eradication of Helicobactor pylori..
2. Acid suppression by:
a. H2 receptor antagonists.
b. Proton pump inhibitors
c. Anti-muscarinic drugs.
3. Neutralisation of secreted acid & pepsin activity by antacids
4. Cytoprotection: Two regimens are currently used for the eradication of Helicobactor pylori, but these will undoubtedly change over the years.

Triple therapy:
1. Bismuth chelate 125 mg 6 hourly for 4 weeks.
2. Metronidazole 400 mg 8 hourly for first week 3. Tetracycline 500 mg 8 hourly for first week.
Alternative therapy:
Omiprazole 20 mg 12-hourly for 4 weeks. plus Amoxacillin 500 mg 6 hourly orally for 7 days. For those who still remain colonised after two treatments. The choice lies between a 3rd attempt with quadruple therapy: Bismuth chelate 125 mg 1 tab QDS daily, plus
- Omiprazole 20 mg 12-hourly for 4 weeks, plus
- Amoxacillin 500 mg 6 hourly orally for 7 days and
- Metronidazole 400 mg 8 hourly for two weeks.
Recently new kits of peptic ulcer treatment are available ‘Helicon kit’ Composition: (in a single strip)
- Lansoprazole 30 mg INN (I cap)
- Amoxacillin 500 mg B.P (2 cap)
- Clarithromycin 500 mg usr (1 rab)
‘Neo kit’
- Composition: (in a single strip)
- Omeprazole 20 mg INN (t cap)
- Metronidazole 400 mg Bp (I rab)
- Clarithromycin 500 mg use (1 tab)
| Drug | How Acts |
| H2 receptor antagonist: ➤ Cimetidine ➤ Ranitidine ➤ Famotidine ➤ Nizatidine ➤ Roxatidine | Reduction of both basal and food stimulated HCI secretion. |
| Proton pump inhibitor: ➤ Omeprazol ➤ Lansoprazole ➤ Pantoprazole ➤ Esomeprazole | Inhibit HCI secretion by inhibiting H+ -K+ pump (proton pump) |
| Anti-muscarinic drugs: ➤ Pirenzipine ➤ Dicyclomine ➤ Propanrhelin. | Inhibit HCl secretion by inhibiting M1 receptor |
| Antacid preparations: ➤ Mg trisillicate ➤ Al(OH)3 gel | Neutralisation of secreted acid No effect on underlying pathology |
| Cytoprotective agents: ➤Bismuth compound ➤Sucralfate ➤ Carboxolone ➤ Prostaglandin E2, 1 | These agents enhance mucosal protection (cytoprotection) |
Drugs that block the H2 receptors are:
- Cimetidine
- Ranitidine
- Famotidine
- Nizatidine
- Roxatidine (Roxatidine acetate hydrochloride)
Pharmacological action of H2 antagonists:
1. Reduce both basal and food stimulated HCI secretion.
2. Healing of ulcer.
3. Anti-androgenic action (cimetidine).
a. Male: Gynaecomastia, impotency
b. Female: Galactorrhoea.
4. Inhibition of cytochrome P-450 oxidase drug metabolizing enzyme; so decrease the metabolism of other drugs:
a. Oral anticoagulants
b. Theophylline
c. Phenytoin
d. Propranolol.
M/A of Ranitidine and Histamine on gastric mucosa:
| RANITIDINE | HISTAMINE |
| Ranitidine/Famotidine ↓ Competitively block the H2 receptor: so histamine cannot acts ↓ Decrcase CAMP formation ↓ Reducrion ol ucid secretion ↓ Healing of ulcer | Histamine ↓ Acts on H2-receptor on parietal cells ↓ Stimulate adenyiate cyclase ↓ Increase cAMP produclion ↓ Acid secretion ↓ Aggravation of ulcer |
Indication of H2 blockers:
1. Peptic ulcer disease (PUD)
- Duodenal ulcer
- Benign gastric ulcer
2. Rellcx oesophagitis.
3. Zollinger Ellison’s syndrome (Hypersecretory condition).
4. Prevention of stress gastritis.
5. Emergency surgery (preanaesthetic medication)
6. Extensive burn (to prevent curling ulcer).
7. Head injury (to prevent Cushing ulcer)
8. Systemic mastocyiosis (hypersecretory state
Adverse effects of H2 blockers:
1. Headache
2. Myalgia
3. Confusion
4. Diarrhoea or constipation
5. Dizziness
6. Weakness
7. In addition to these cimetidine causes:
8. Gynaecomastia
9. Impotency
Dose and administration
1. Ranitidine Tab. 150 mg 1+0+1 for 6-8 weeks Maintenance dose 0+0+1
2. Famotidine Tab.40 mg 0+0+1 (bed time) for 4-8 weeks only Tab. 20 mg Maintenance dose 0+0+1
3. Ranitidine: 10 times more potent than Cimetidine.
4. Famotidine: 8 times more potent than Ranitidine.
Famotidine
a. Long acting H2 receptor antagoilist.
b. Faster pain relief.
c. Faster ulcer healing..
d. Reduce recurrence rate.
e. Better patient compliance.
f. No drug interactiou of clinical signitionce.
Omeprazole
a. Proton pump inhibitor
b. It is a weak base; prodrug.
c. Inactive at neutral PH, activated in PH <3 by protonution.
d. Pharmacological action: inhibits both basal cannel focal stimulated acid secretion.
e. It is effective in patients resistant to H₂ receptor antagonist
Mechanism of action of omeprazole
Omeprazole is a proton-pump inhibitor. It is-reversibly inhibits the enzyme H+ -K+-ATPase (this enzyme is located in the luminal wall of the parietal cells). This H+ -K+-ATPase enzyme is responsible for exchange of H-K pump is the terminal pathway of acid secreting process in the stomach.
Indication of omeprazole
1. Zollinger-Eliison syndrome.
2. Ulcerative-reflux esophagitis
3. Active duodenal ulcer.
4. Multiple endocrine neoplasias
Adverse effects of omeprazole
1. Carcinoid tumour (prolong rise)
2. Nausea, vomiting, diarrhoea.
3. Headache.
4. Pirenzipine
5. Propantheline
6. Dicyclomine
Gastrin producing tumour of pancreas, causing hyper secretion of-gastric acid and severe peptic ulceration. Zollinger-Ellison syndrome is a rare condition in which one or more tumors form in your pancreas or the upper part of your small intestine (duodenum).

These tumors, called gastrinomas, secrete large amounts of the hormone gastrin, which causes your stomach to produce too much acid. The excess acid then leads to peptic ulcers, as well as to diarrhea and other symptoms. Zollinger-Ellison syndrome (ZES) is rare. The disease may occur at any time in life, but people usually find out they’re affected between ages 20 and 50. Medications to reduce stomach acid and heal the ulcers are the usual treatment for Zollinger-Ellison syndrome.
Symptoms
Signs and symptoms of Zollinger-Ellison syndrome may include:
- Abdominal pain
- Diarrhea
- Burning, aching, gnawing or discomfort in your upper abdomen
- Acid reflux and heartburn
- Nausea and vomiting
- Bleeding in your digestive tract
- Unintended weight loss
- Decreased appetite
Pirenzepine
They are anti-secretory, anti-spasmodic agents. Pirenzipine has high affinity for N41 receptor in autonomic ganglia.
Pirenzipine
↓
Selectively block the Mi receptor in autonomic ganglia
↓
Decrease parasympathetic outflow to the gut.
↓
Decrease secretion (anti-secretory) Decrease spasm (anti-spasmodic)
Clinical uses:
1. Duodenal ulcer.
2. Inevitable borvei syndrome
3. Diverticular disease.
Adverse effects
1. Dry mouth
2. Blurred vision.
3. Constipation
4. Urinary retention
Read more: