
Iodine Deficiency Disorder (IDDs)/ Goitre – This book covers the entire syllabus of “Nutrition and Dietetics” prescribed by BNMC-for all Diploma in Nursing Science and Midwifery students. We tried to accommodate latest information and topics.
This book is examination friendly setup according to the teachers’ lectures and examination’s questions. At the end of the book previous university questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourished. The unique way of presentation may make your reading of the book a pleasurable experience.
Iodine Deficiency Disorder (IDDs)/ Goitre
Definition of Endemic Goitre:
When goitre occurs in a significant number of people (more than 10% of population) in a defined geographic area, it is known as endemic goiter.
Definition of Goitre:
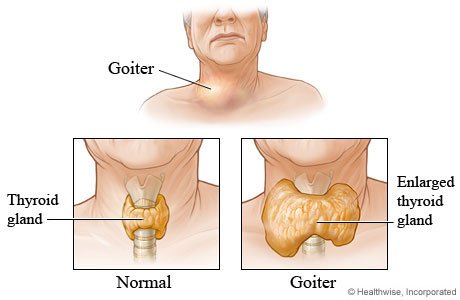
A goitre, or goiter, is a swelling in the neck resulting from an enlarged thyroid gland. Goitre can be associated with a thyroid that is not functioning properly.
Worldwide, over 90% of goitre cases are caused by iodine deficiency.
or
Goitre (sometimes spelled “goiter”) is a swelling of the thyroid gland that causes a lump in the front of the neck. The lump will move up and down when swallow.
or
Any enlargement of the thyroid gland is called goiter.

Geographical Distribution:
The number of people in Bangladesh, who have visible goitre is more than 15 million.
- Andes.
- Himalyas.
- Central Africa.
- Bangladesh- Rangpur, Dinajpur, Bogra, Tangail, Jamalpur, Mymensingh.
Iodine Deficiency Disorder Develop By –
1. If there is not enough iodine in food, the level of iodine in the blood falls and stores of iodine in the thyroid gland are used up
2. The thyroid gland enlarges to collect more iodine from the blood. The enlarged gland is called a goitre.
3. If the enlarged thyroid gland produces enough thyroid hormone, the person’s body works normally the goitre is the only abnormality.
4. If the gland fails to produce enough thyroid hormone, the person becomes hypothyroid.
Causes of Thyroid Enlargement (Goiter):
A. Diffuse goiter:
- Simple goiter.
- Graves’ disease
- Hashimoto’s thyroiditis.
- Iodine deficiency (endemic goitre).
- Drugs: Iodine, amiodarone, lithium.
- Transient thyroiditis.
- Suppurative thyroiditis.
- Dyshormonogenesis.
- Infiltrative: Amyloidosis, sarcoidosis etc.
- Riedel’s thyroiditis.
B. Multi-nodular goiter.
C. Solitary nodule;
- Simple cyst.
- Colloid nodule.
- Follicular adenoma.
- Papillary carcinoma
- Follicular carcinoma.
- Medullary cell carcinoma.
- Anaplastic carcinoma.
- Lymphoma.
- Metastasis
Types of Goiter:
- Grade 0: No goitre. Lobes smaller than end joint of thumb.
- Grade I A: Thyroid lobes larger than ends of thumbs.
- Grade IB: Thyroid gland visible with head bent back.
- Grade 2: Thyroid gland visible with head in normal position.
- Grade 3: Thyroid gland visible from about 10 metres.
In A Community Survey:
- Grade 2 and 3 are called visible goitre.
- Grade 1A, 1B, with grades 2 and 3 are called total goitre
Clinical Classification:
- Grade 0- Absence of goiter.
- Grade 1 – Only palpable, not visible in normal neck position.
- Grade 2- Visible in normal position.
Features of Toxicity of a Goiter:
Symptoms:
- Weight loss, despite normal or increased appetite.
- Heat intolerance.
- Palpitation.
- Tremor.
- Increased sweating.
- Chronic diarrhoea.
Signs:
- Warm & sweaty hands.
- Tachycardia and irregularly irregular pulse.
- Ocular signs – Exophthalmos, lid lag, lid reatraction.
- Pre-tibial myxoedema.
Diagnosis:
History: History of endemic area.
Physical examination:
➤ Diffuse goiter: Examination of thyroid gland reveals –
- Symmetrical enlargement.
- Non-tender.
- Consistency soft.
- No lymphadenopathy.
- No bruit.
- Surface smooth.
➤ Multinodular goiter: Examination of thyroid gland reveals –
- Variable size and shape.
- Non-tender.
- Consistency firm.
- Surface nodular or multilobulated.
Investigations:
➤ Diffuse goiter:
- T3 and 14: Normal
- TSH: Normal
➤ Multinodular goiter:
- T3 and T4: Normal or raised.
- TSH: Normal or undetectable

Treatment:
➤ Diffuse goiter:
- Usually treatment is not required.
- In most cases goiter regresses.
➤ Multinodular goiter:
- If small, then treatment is not necessary.
- If there is a progression to toxic multinodular goiter, then partial thyroidectomy.
Prevention of Iodine Deficiency Disorders:
1. Iodized salt:
- It is not less than 30 ppm at the production point.
- It is not less than 15 ppm of iodine at the consumer level.
- Iodized oil, oral: The oral administration of iodine as iodized oil or as sodium iodate tablets is technically simpler than the injection method.
2. Iodine monitoring:
- Determination of iodine excretion.
- Determination of iodine in water, soil and food.
- Determination of iodine in salt for quality control.
3. Manpower: It is vital for the success of control that health workers and others engaged in the program be fully trained in all aspects of goitre control including legal enforcement and public education.
4. Mass communication: Mass communication is a powerful tool for nutrition education. It should be fully used in goitre control work.
5. Hazards of iodization: A mild increase in incidence of thyrotoxicosis has now been described following iodized salt program.
Examination of a Goiter:
1. Stand or sit facing the person.
2. Place our two thumbs on either side of the person’s trachea, several centimeters below the larynx (voice box). 3. Roll our thumbs gently over the thyroid (Which lies next to the trachea). This is called ‘palpation’.
4. If each lobe of the thyroid is smaller than the end joint of the person’s thumb, there is no goitre.
5. If one or both lobes is larger than the end joint of the person’s thumb, then there is a goitre.
6. Ask the person to bend their head back and look upwards. Try to see the goitre.
7. Ask the person to look straight forward and try to see the goitre again.
8. Notice if we can see the goitre from a distance of about 10 metres or only from close up