Definition of Episiotomy – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Definition of Episiotomy
Episiotomy:
It is a surgically planned incision on the perineum & the posterior vaginal wall during the second stage of labour.It is in fact an inflicted 2nd degree perineal injury. It is the most common obstetric operation performed.
Or
Episiotomy, also known as perineotomy, is a surgical incision of the perineum and the posterior vaginal wall generally done by a midwife or obstetrician during second stage of labor to quickly enlarge the opening for the baby to pass through.
Indications of episiotomy:
1. In case of rigid / inelastic perineum:
➤ Elderly primigravida – causes arrest or delay in descent of the presenting part.
2. Anticipating perineal tear:
➤ Big baby.
➤ Face to pubis delivery.
➤ Breech delivery.
➤ Shoulder dystocia
1. Operative delivery:
➤ Forceps delivery.
➤ Ventouse delivery.
2. Previous perineal surgery:
➤ Previous pelvic floor repair.
➤ Previous reconstructive surgery
[Ref-D. C. Dutta’s Obs/9/528]
4 indications of episiotomy:
1. Breech presentation.
2. Big baby.
3. Elderly primigravida.
4. Shoulder dystocia.
Benefits of episiotomy:
Maternal:
1. A clear & controlled incision is easy to repair & heals better than a lacerated wound that might occur otherwise.
2. Reduction in the duration of second stage.
3. Reduction of trauma to the pelvic floor muscles that reduces the incidence of prolapse & perhaps urinary incontinence.
Fetal:
1. Minimizes intra-cranial injuries in premature babies or after-coming head of breech.
[Ref-D. C. Dutta’s Obs/9/528)
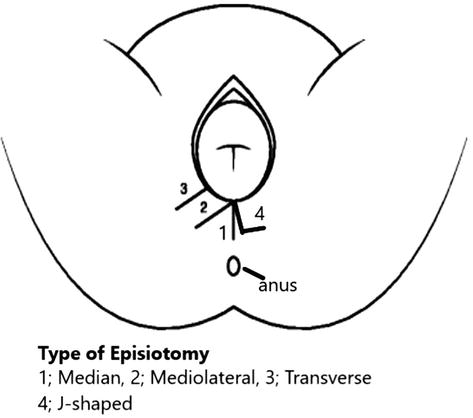
Medio-lateral episiotomy:
The incision is made downwards & outwards from the midpoint of the fourchette either to the right or Left (preferably on the right side to avoid injury to the rectum). It is directed diagonally in a straight line which runs about 2.5 cm away from the anus (midpoint between anus & ischial tuberosity).
Median episiotomy:
The incision commences from the center of the fourchefte &extends posteriorly along the midline for about 2.5 cm.
Lateral episiotomy: The incision starts from about I cm away from the center of
fourchette&extends laterally. It is not practiced due to chance of injury to the duct of Bartholin’s gland, disfigurement of the perineum and excessive bleeding.
“J” shaped episiotomy: This incision begins in the centre of fourchette& directed posteriorly along the midline for about 1.5 cm and then directed downwards & outwards along 5 or 7 o0, clock position to avoid the anal sphincter. Apposition is not perfect & the repaired-wound tends to be puckered. This is also not done widely.
Procedures of episiotomy:
1. Perineum is cleaned thoroughly with antiseptic solution (10% povidone iodine) & draped properly.
2. Then the perineal skin is infiltrated with 1% 10-20 ml Xylocaine in a fan shaped manner starting from the midpoint of the fourchette.
3. An incision is made by curved scissors under the guidance of 2 fingers placed between the posterior vaginal wall & the presenting part.
Following structures are cut from inside outwards:
➤ Posterior vaginal wall.
➤ Deep & superficial transverse perineal muscles, bulbo-spongiosus& part of the levatorani muscle.
➤ Fascia covering the muscles.
➤ Transverse perineal branches ofpudendal vessels & nerves.
➤ Subcutaneous tissue & skin.
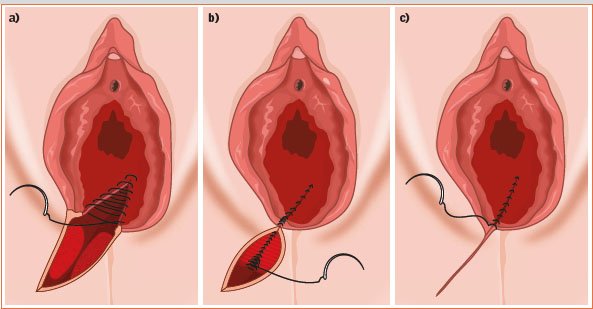
4. After completion of the 3rd stage of labour, the vagina & cervix are to be inspected for any injury & then repair is to be done started from a point beyond the apex of the incision in the posterior vaginal wall in a continuous fashion up to the introitus.
5. Three or four interrupted sutures are then placed in the muscle.
6. Skin & subcutaneous tissues are approximated by interrupted stitches using catgut (or silk) with a cutting body needle.
[Ref– D. C. Dutta’s Obs/9/529-530]
Structures eut during episiotomy:
- Posterior vaginal wall.
- Superior & deep transverse perineal muscles, bulbospongiosus & part of levatorani.
- Fascia covering those muscles.
- Transverse perineal branches of pudendal vessels & nerves.
- Subcutaneous tissues & skin.
Post-operative care of episiotomy injury:
Dressing:
The wound is to be dressed each time following urination & defecation to keep the area clean & dry. The dressing is done by swabbing with cotton-swabs soaked in antiseptic solution, followed by application of antiseptic powder or ointment. During dressing, the attendant should wear a mask.
Comfort:
To relieve pain in the area, MgSO4 compress or application of infra-red heat may be used,2 Analgesic drugs (aspirin) may be given as and when required.
Ambulance:
After 24 hours the patient is allowed to move out of her bed.
Removal of the stich:
If the wound is stitched with cat gut or dexon the stitches will be absorbed and don’t need to remove. But if non-absorbable materials like silk or nylon is used. The stitches are to be cut on 7th day. The number of stitches removed should be checked with the record of the stitches given.
[Ref-D. C. Dutta’s Obs/9h/530]
Complications of episiotomy:
Immediate complications:
1. Extension of the incision which may involve anus sphincter.
2. Haemorrhage: Excessive bleeding may occur if the episiotomy is given too soon.
3. Vulval haematoma.
4. Wound infection (throbbing pain in the perineum, rise in temperature and the wound area looks moist, red & swollen).
5. Wound dehiscence.
6. Recto-vaginal fistula.
Remote:
1. Dyspareunia (due to a painful perineal scar).
2. Perineal laceration.
3. Bartholin’s cyst.
4. Deficient perineum.
5. Recto-vaginal fistula.
6. Scar endometriosis.