
Definition of Meningitis – Health of the children has been considered as the vital importance to all societies because children are the basic resource for the future of humankind. Nursing care of children is concerned for both the health of the children and for the illnesses that affect their growth and development. The increasing complexity of medical and nursing science has created a need for special area of child care, i.e. pediatric nursing.
Pediatric nursing is the specialized area of nursing practice concerning the care of children during wellness and illness. It includes preventive, promotive, curative and rehabilitative care of children. It emphasizes on all round development of body, mind and spirit of the growing individual. Thus, pediatric nursing involves in giving assistance, care and support to the growing and developing children to achieve their individual potential for functioning with fullest capacity.
Definition of Meningitis
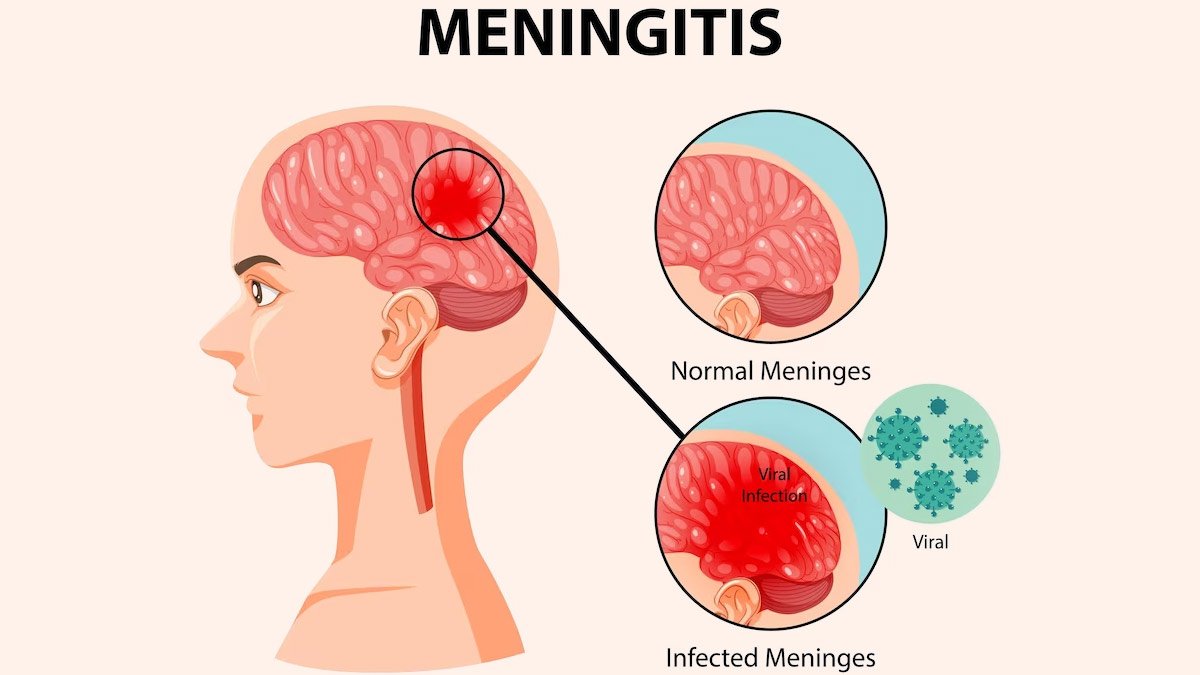
Meningitis is an acute inflammation of the protective membranes covering the brain and spinal cord, known collectively as the meninges. The most common symptoms are fever, headache, and neck stiffness. Other symptoms include confusion or altered consciousness, vomiting, and an inability to tolerate light or loud noises.
Young children often exhibit only nonspecific symptoms, such as irritability, drowsiness, or poor feeding. If a rash is present, it may indicate a particular cause of meningitis; for instance, meningitis caused by meningococcal bacteria may be accompanied by a characteristic rash.
The inflammation may be caused by infection with viruses, bacteria, or other microorganisms, and less commonly by certain drugs. Meningitis can be life-threatening because of the inflammation’s proximity to the brain and spinal cord; therefore, the condition is classified as a medical emergency.
A lumbar puncture can diagnose or exclude meningitis. A needle is inserted into the spinal canal to collect a sample of cerebrospinal fluid (CSF) that envelops the brain and spinal cord. The CSF is examined in a medical laboratory.
Definition of Meningitis:
Meningitis refers to inflammation of the meninges overlying brain and spinal cord.
Or
Inflammation of meninges overlying brain and spinal cord present with characteristic combination of pyrexia & headache.
(Ref-Davidson’s Medicine/224/1202)
Causes of Meningitis:
A. Infective causes of meningitis
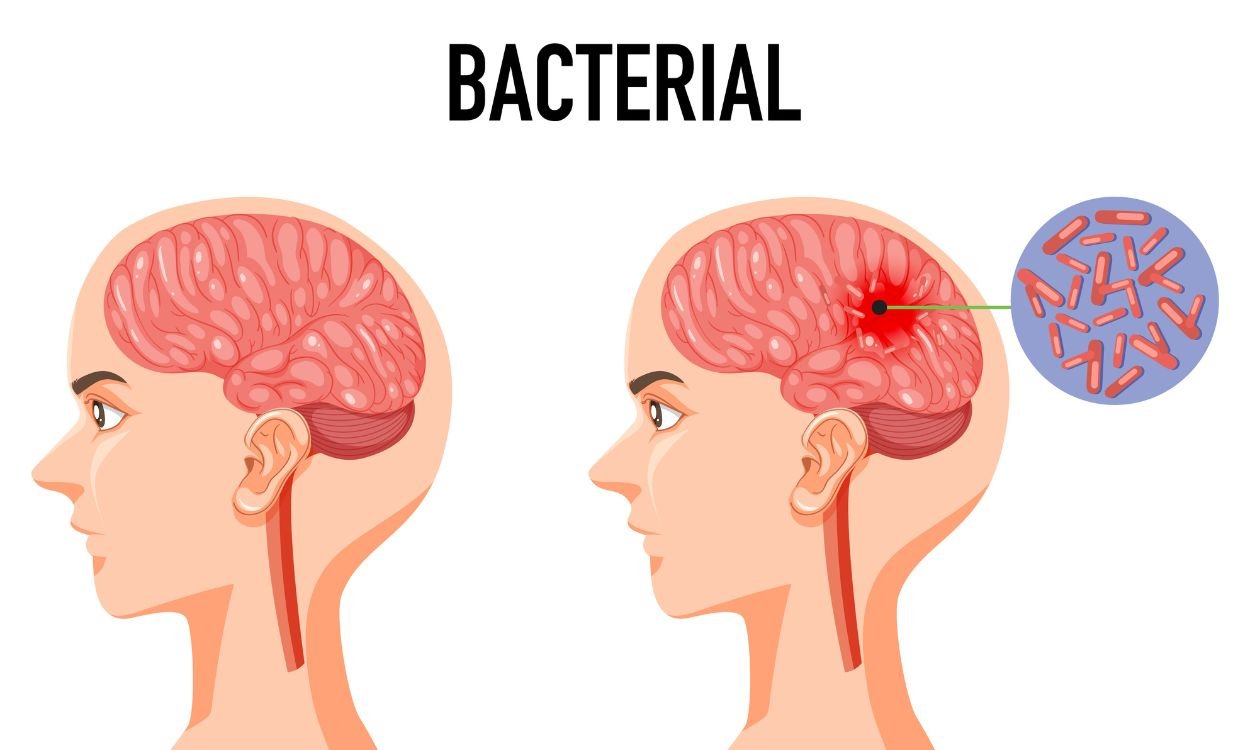
a) Bacterial causes
According to Age of Onset
| Age of onset | Common | Less common |
| A. Neonate |
|
|
| B. Pre-school child |
|
|
| C. Older child and adult |
|
|
b) Viruses:
- Enteroviruses (echo, Coxsackie, polio)
- Mumps
- Influenza
- Herpes simplex
- Varicella zoster
- Epstein-Barr
- HIV
- Lymphocytic choriomeningitis
- Mollaret’s meningitis (HSV type 2)
c) Protozoa and parasites:
- Toxoplasma
- Amoeba
- Cysticercus
- Cryptococcus neoformans
d) Fungi:
- Candida
- Histoplasma
- Blastomyces
- Coccidioides
- Sporothrix
B. Non-infective (‘sterile’):
a) Malignant disease:
- Breast cancer
- Bronchial cancer
- Leukaemia
- Lymphoma
b) Inflammatory disease (may be recurrent):
- Sarcoidosis
- SLE
- Behcet’s disease
(Ref-Davidson’s Medicine/224/1205)
Types of Meningitis
| A. According to micro- organism: | a) Pyogenic or bacterial meningitis. b) Tuberculous meningitis. c) Viral meningitis. d) Fungal meningitis. |
| B. According to durations: | a) Acute meningitis b) Chronic meningitis |
| C. According to pus formation: | a) Pyogenic or bacterial meningitis: Forms pus. b) Aseptic meningitis: (Tuberculosis meningitis. Viral meningitis. Fungal meningitis & parasite): Not form pus. c) Non-infective (‘sterile’) meningitis:
|
Pathogenesis of Bacterial Meningitis
From infection in the ear or skull fracture or sinus or from other bacteraemic illness
↓
Leptomeninges
↓
Congested and infiltrated with inflammatory cells
↓
A thin layer of pus forms and this may later organize to form adhesions
↓
Obstruction to the free flow of CSF leading to hydrocaphalus and produces other signs symptoms of meningitis.
Management of Pyogenic/ Bacterial Meningitis:
Clinical Features of Bacterial Meningitis:
a) New born:
- Vacant stare
- Fever/hypothermia
- Drowsiness/ irritability
- Vomiting
- Reluctance to feed
- Poor tone and poor cry
- Convulsion
- Fontanelle may bulge
- Kernig’s sing may present
- Neck rigidity absent
b) Older and adult:
- Headache
- Drowsiness
- Fever
- Vomiting
- Restlessness
- Irritability
- Coma, convulsion
- Cranial nerve palsies
- Neck rigidity, kernig’s sing and Brudzinskis sign may be positive
Investigations:
- CSF study, cytology, biochemistry, gram stain, culture
- Serological tests
- Cranial ultrasound scan when fontanels are patient (up to 18 month)
- Blood for CBC & C/S
- CT scan to exclude more lesion: cerebral abscess
Treatment of Meningitis
A. In 1st 3 months of life
- a) Inj. ampicillin ( 400mg / k * g / d * ay I/V, 4 divided doses) plus.
- b) Inj. cefotaxime ( 200nag / k * g / d * ay , 4 divided dose I/V) or
- c) Inj. ceftriaxone ( 100mg / k * g / d * ay once daily I/V).
B. Beyond 3 months of age :
- a) Inj. Ampicillin Inj. plus chloramphenicol ( 100mg / k * g / d * ay 4 divided dose I/V or I/M).
- b) Inj. crystalline penicilin (300, 0U / k * g / 24 * hr) for 5-7 day is the treatment complicated meningucoccal meningitis.
- c) Duration of therapy for meningitis is generally 10-14 day (or 14-21 days in Gram negative bacillus infection).
C. Anti-inflammatory therapy
- a) IV dexamethasone in a dose 0.15 mg/kg/dose given I/V hrly for 2 days.
- b) It should be given 15 min before antibiotic treatment.
D. Symptomatic treatment
- a) Parcetamol
- b) Per rectally diazepam (05 mg/kg/dose)
- c) Subsequently phenytoin 15 – 20mg / k * g loading dose followed by 5 mg/kg/24hrs as maintenance dose car be used.
E. Treatment of complications:
- a) Increased intracranial pressure can be treated with intravenous mannitol (0.5
- b) mg/kg/IV infusion) and intravenous furosemide.
- c) Shock should be treated with volume expander.
(Ref by- M. R. Khan 4th edition)
Complication of Meningitis:
A. Immediate:
- Increase intracranial pressure (ICP)
- Cranial nerve palsies
- Cerebral or cerebellar herniation
- Subdural effusion
- Empyema
- Hydrocephalus
- SIADH
- Shock DIC
- Brain abscess
B. Late:
- Permanent brain damage
- Cerebral palsy
- Mental retardation
- Epilepsy
- Deafness
- Hydrocephalus
Differentiating Features of Different Meningitis:
| Traits | Normal findings | Acute bacterial meningitis | Viral meningitis | Tuberculous meningitis |
| A. Pressure | 50-180 mm of water | Normal /increased | Normal | Normal/increased |
| B. Colour | Clear | Cloudy | Clear | Clear/cloudy/Spider web/fine clot |
| C. Red cell count | 0-4×106/1 | Normal | Normal | Normal |
| D. White cell count | 0-4×106/1 | 1000-5000 polymorphs | 10-2000 lymphocytes | 50-5000 lymphocytes |
| E. Glucose | > 60% of blood level | Decreased | Normal | Decreased |
| F. Protein | <0.45 g/1 | Increased | Normal/increased | Increased |
| G. Oligoclonal bands | Negative | Can be positive | Can be positive | Can be positive |
Nursing Management of Meningitis:
Nursing management of the patient with meningitis includes the following:
Nursing Assessment
Assessment of the patient with bacterial meningitis include-
- Neurologic status. Neurologic status and vital signs are continually assessed.
- Pulse oximetry and arterial blood gas values. These values are used to quickly identify the need for respiratory support.
Nursing Diagnosis
- Based on the assessment data, major nursing diagnoses include:
- Risk for Infection related to contagious nature of organism.
- Acute Pain related to headache, fever, neck pain secondary to meningeal irritation.
- Impaired Physical Mobility related to intravenous infusion, nuchal rigidity and restraining devices.
- Activity Intolerance related to fatigue and malaise secondary to infection.
- Risk for Impaired Skin Integrity related to immobility, dehydration, and diaphoresis.
- Risk for Injury related to restlessness and disorientation secondary to meningeal irritation.
- Interrupted Family Process related to critical nature of situation and uncertain prognosis. .
- Anxiety related to treatment and risk of death.
- Risk for Ineffective Therapeutic Regimen Management
Nursing Care Planning & Goals
Goals for a patient with bacterial meningitis include:
- Protection against injury.
- Prevention of infection.
- Restoring normal cognitive functions.
- Prevention of complications.
Nursing Interventions
Important components of nursing care include the following measures:
- Assess neurologic status and vital signs constantly. Determine oxygenation from arterial blood gas values and pulse oximetry.
- Insert cuffed endotracheal tube (or tracheostomy), and position patient on mechanical ventilation as prescribed.
- Assess blood pressure. (Usually monitored using an arterial line) for incipient shock, which precedes cardiac or respiratory failure.
- Rapid IV fluid replacement may be prescribed, but take care not to overhydrate patient because of risk of cerebral edema.
- Reduce high fever to decrease load on heart and brain from oxygen demands.
- Protect the patient from injury secondary to seizure activity or altered level of consciousness (LOC).
- Monitor daily body weight, serum electrolytes; and urine volume, specific gravity, and osmolality, especially if syndrome of inappropriate antidiuretic hormone (SIADH) is suspected.
- Prevent complications associated with immobility, such as pressure and pneumonia.
- Institute infection control precautions until 24 hours after initiation of antibiotic therapy (oral and nasal discharge is considered infectious).
- Inform family about patient’s condition and permit family to see patient at appropriate intervals.
Evaluation
Expected patient outcomes include:
- Avoidance of injury.
- Avoidance of infection.
- Restoration of normal cognitive functions.
- Prevention of complications.