
External Fixations – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
External Fixations
External fixation is the method of fixing fracture with a cluster of pins connected to external bars.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, edition,p-78)
Or
External fixation allows stabilization of a fracture at a distance from the fracture site without soft tissue damage.
Or
External fixation is a mechanical construction to hold a fracture. Each side of the fracture is coupled to the fixator and the major part of the device is external to the skin. The couple to the bone is via either half pins (that is stiff metal fords typically 5-6 mm in diameter) or tensioned wires (typically 1.8 mm in diameter), which are than secured to frame by clamps.
[Ref-Bailey & Love’s, “Short Practice of Surgery”, 25th edition, P-364)
Classification of external fixation:
A) On the basis of method of fixation:
1. Simple pin fixator.
2. Clamp pin fixatior.
3. Ring pin fixator.

B) On the basis of frame design
1) Unilateral frame: this is the simplest external fixator frame. Four pins, two above, and two below the fracture passed through the bone and fixed to a frame.
2) Bilateral frame: This improves the frame stiffness and helps in better control of bending and torsional forces.
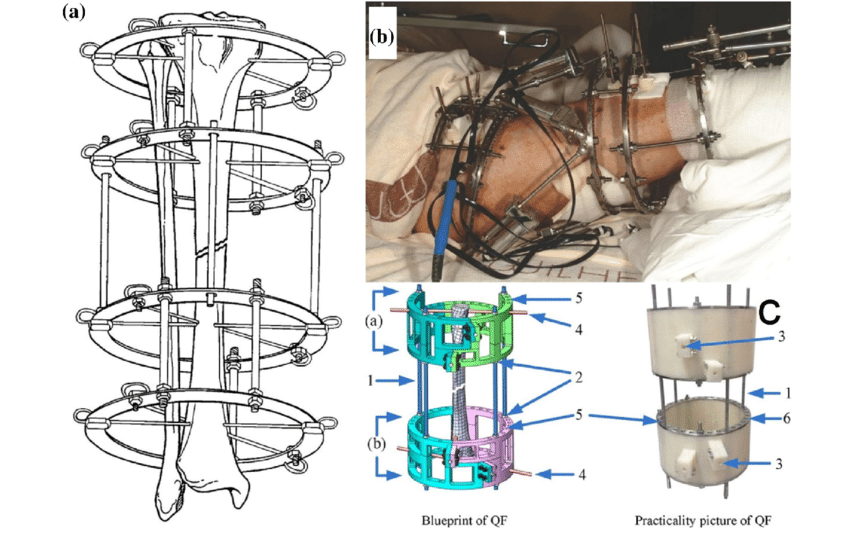
3) Ring fixators: This has been dealt with separately and multiplaner.
4) Hybrid fixators: This helps to combine the advantage of uniplaner and multiplaner external fixator devices. They are especially useful in fixing periarticular fracture.
[Ref- John Ebnezar’s, “Textbook of Orthopedics”, edition,p-79+ Lippincott’s, adult orthopaedic nursing]
Indications of external fixation:
1. Emergency use of external fixation:
i. Patients with massive trauma
ii. Unstable pelvic fracture, Acetabular fracture
iii. Neurovascular compromise.
2. Non-emergency use of external fixation:
i) Fracture where hone deficit.
ii) Treating fracture with a bone loss,
iii) Soft tissue damage.
iv) Leg lengthening
v) Correction of deformity.
vi) Fracture associated with burns
vii) To treat grossly contaminated wound, unstable fracture.
[Ref-Bailey & Love’s, “Short Practice of Surgery”, 25 edition.p-364]
Contraindications of external fixation:
1. Patient with compromised immune system
2. Non compliant patient who would not be able to ensure proper wire and pin care
3. Pre-existing internal fixation that prohibits proper wire or pin placement
4. Bone pathology precluding pin fixation
Roles of external fixation in the management of open fracture:
1. To stabilize fracture fragments.
2. To allow daily wound inspection.
3. It allow regular dressing of the wound.
4. It provide procedure like skin grafting to cover the wound.
5. Allow heal in the soft tissue.
Component of external fixator: External fixator consist of 3 basic components-
1) Pin
2) Clamps
3) External rods.
Pin:
Pins are passed through the bones at different levels and fixed to an external frame by the clamps,
Types of pins:
1. Half pins: Commonlu used.
2. Full pins: These are centrally threated and transfix the entire bone. Diameter: 4-5 mm.
3. Thins pins: Used in circular external fixators.
4. Cortical pins: Here the thread diameter increases from the tip to the shaft.
5. Self drilling pins.
6. Hydroxyapatile coated pins.

[Ref- John Ebnezar’s, “Textbook of Orthopedics”, edition.p-79/]
Clamps:
These connect the pins to the rods.
Types of clamps:
1. Simple clamps: This connect single single pin or wires to the rods or ring
2. Modules clamps: These connect several pins as clusters.

[Ref- John Ebnezar’s, “Textbook of Orthopedics”, edition.p-79]
External rod:
These connect the cluster of pins through various clamps.
Modes of action of external fixator:
There are many mode of action Which maintain stabilization during fixation:
1) Compression forces: These forces help to stabilize certain transverse fractures and for compression arthrodesis.
2) Distraction forces: These make the ligaments, muscles capsules and other soft tissues by ligamentotaxis. These forces helps in reduction and retention of the fracture fragments. Commonly used in distal radial, tibial plateau and pilon fractures.
3) Neutralization fractures: This provides neutralizing forces across the fracture site.
4) Angulation forces: These are used to bend rotate, and convert the angulations.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, edition.p-80]
Biotechnical principles of External fixation:
Following are the biotechnical principles which influence the mechanical stability of the external fixator:
1) Pin size: Greater the pin size, Greater the stability of fixation.
2) Pin number: More number of pins ensures better stability.
3) Pin placement: The placement of pins include very near on either side of the fracture site or farthest away from the fractures. This is known as the “Near far construct”.
4) Rod placement: Rod placed closer to the bone gives better stability. Double stacking the rods also. increase stability.
5) Clamps: The rigidity of fixators decreases considerabely if the clamps do not hold the pins firmly. Hence periodic tightening of the clamps is a useful and effective practice.
[Ref-John Ebnezar’s, “Textbook of Orthopedics”, edition, p-801]
Advantages of external fixation:
1. No interference with fracture site.
2. Adjustable after application: alignment, biomechanics.
3. Soft tissue accessible for plastic surgery.
4. Rapid stabilization of fracture.
5. Hardware easy to remove.
Disadvantages of external fixation:
1. Pin site infection.
2. Interferes with plastic surgical procedures.
3. Soft tissue tethering.
4. Cumbersome for the patient
Complications of external fixation:
1.Pin loosening.
2. Pin migration.
3. Pin breakage.
4.Pin tract infection.
5.Limitation of joint motion.
6. Neurovascular damage.
7. Compartmental syndrome.
8. Chronic osteomyelitis.
9.Septic arthritis. (If pin fixed near joint)
10. Soft tissue contracture.
11. Malunion.
12. Delayed union/Non-union.

[Ref- John Ebnezar’s, “Textbook of Orthopedics”, 4 edition, p-80]
Nursing management a case of external fixation patients in orthopedic ward:
A) Assessment:
1. Assess neurological status of patients, and level of consciousness.
2. Check vital signs
3. Assess pan on the basis of pain scale.
4. Assess the operative site-Clean, tightness of pins, any signs of infection,
5. Check dressing site-blood oozing, Soaked or dry dressing.
6. Determine patients level of anxiety.
7. Assess functioning of other body system.
B) Nursing diagnosis:
1) Pain and discomfort related to bone and soft tissue trauma.
2) Impaired physical mobility related to instability of the tibia and fibula.
3) Increased anxiety related to appearance of external fixator device on the leg.
4) Risk of developing secondary infection in pin sites due to lack of care.
5) Knowledge deficit related to cure of fixator and rehabilitation process.
C) Nursing intervention:
1) Alleviating pain:
- Assess the pain status.
- Elevate the extremity to reduce pain and circulation.
- Regular dressing of pin sites by povisep solutions.
- Relaxation technique, such as deep breathing, reading book, listening song Immobilization of the join to reduce pressure on the injured site.
- Give analgesics according to doctor’s order and monitor pain relief
2) Increase physical mobility:
- Elevate the leg with external fixator using pillows.
- Do not place your hand under the fracture site to move the leg.
- Active and Passive ROM should be applied all unaffected joint.
- Teach the patient about quadriceps exercise.
- Teach the patients of crutch walking.
- Assist the patient during movement.
- Avoid weight bearing activity in the leg.
- Trained the patient how to get up and down in chairs.
3) Releiving anxiety:
- Observe the signs of depression
- Talk with the patient about care and patients co-operations
- Encourage the patients to ask freely.
- Observe sleeping pattern if insomnia consult with doctors.
- Encourage the family members to cop e with the problem and adjust with negative thought.
- Encourage the patient to deep breathing when anxiety is more.
4) Prevention of infection:
a) Care to pin sites:
- Inspect the pin sites everyday.
- Note skin tension in pin sites.
- Note placement of pins.
- Report loosing pins. And loosing pin should be replaced.
- Note any signs of infection if there is discharge give sterile dressing.
b) Wound care:
- Regular inspect of the skin.
- Change dressing everyday
- Clean the woun with povisep solution.
- Avoid touching the wound in open hand.
- Always use of sterile gauze, cotton, bandage.netea
- During dressing remove dead cells, if present.
- If infection or pus in the wound wash with 50% N/S +50% H2O2
c) Sterile technique:
- Use of sterile instrument, gauze.
- Encourage patients to maintain personal hygiene.
- Change bed cloths regularly.
- Keep area of external fixator clean and dry.
d) Pharmacological care:
- Investigate Blood for TC,DC, ESR, RBS, Urine R/M/E etc.
- Give prophylactic antibiotic to prevent development of secondary infections.
- Use of topical antibiotic (If necessary). Control blood sugar if the pts is DM.
5) Patients educations:
- Advise the clean fixator regularly.
- Avoid weight bearing activity.
- Taking regular medications.
- Taking Calcium and Vitamin containing diet.
- Encourage the patients to follow rehabilitation regim.
[Ref: Lippincott, Adult orthopaedic nursing, P-207]