Fracture of Patella – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Fracture of Patella
Functions of patella:
1) Increases the mechanical advantage of quadriceps tendon by increasing the efficiency of extensor mechanism by as much as 50 percent due to increased level arm.
2) To aid in the nourishment of articular cartilage.
3) To protect the femoral condyles from injury.
4) Acts as a hydraulic brake.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-258]
Classifications of fracture of patella:
A) Undisplaced :
1) Transverse fracture these account for nearly 50-80 percent of cases. About 80 percent occur in the middle-third.
2) Stellate fracture.
3) Vertical fracture.
B) Displaced: If displacement is >3 mm and if articular incongruity > 2 mm.
1) Transverse involving upper or lower poles (50-85%).
2) Oblique fracture.
3) Vertical fracture (12-27%).
4) Comminuted fracture (30-35%). 5) Polar-could be proximal or distal.
6) Osteochondral fractures.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-259]
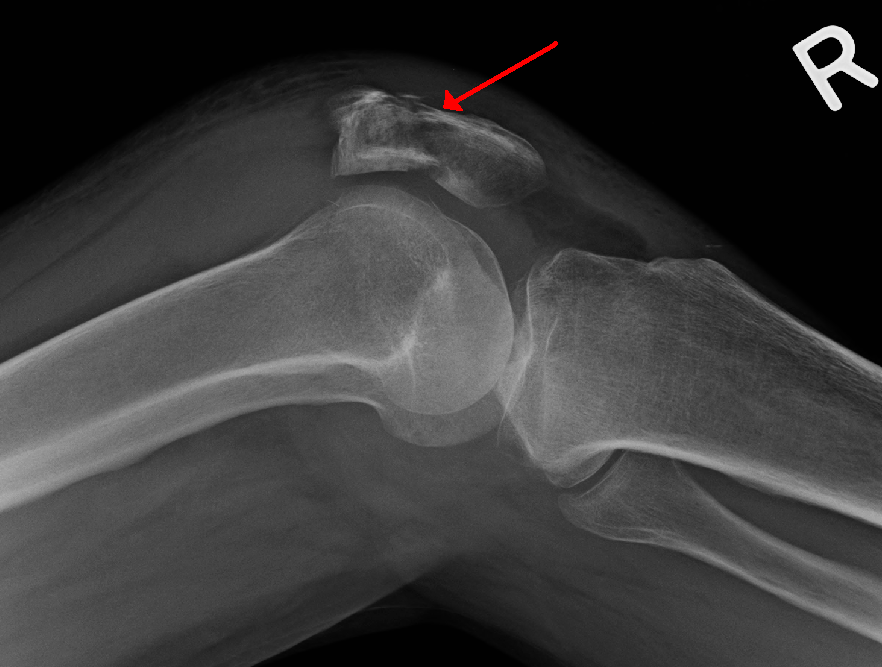
Clinical features of fracture of patella:
1. Hi story of trauma.
2. Pain & swelling at the knee joint.
3. The patient is unable to extend the knee.
4. Both the active & passive movements are restricted.
5. On examination :
a) There could be a palpable gap.
b) Tenderness.
c) Signs of effusion.
d) A positive patellar tap.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-259]

Management of fracture of patella:
A) Undisplaced Fracture: Non operative treatment will produce good results in undisplaced fracture and if displacement is less than 1-2 mm and in intact extensor mechanism and minimal articular step-off (<1-2 mm) and the methods include:
1. Compression bandage.
2. Ice applications.
3. Aspiration of hemarthrosis.
4. Cylindrical cast in extension or long leg cast for 4-6 weeks.
5. Functional cast brace is also effective.
6. The patient is advised early weight bearing and quardriceps exercises.
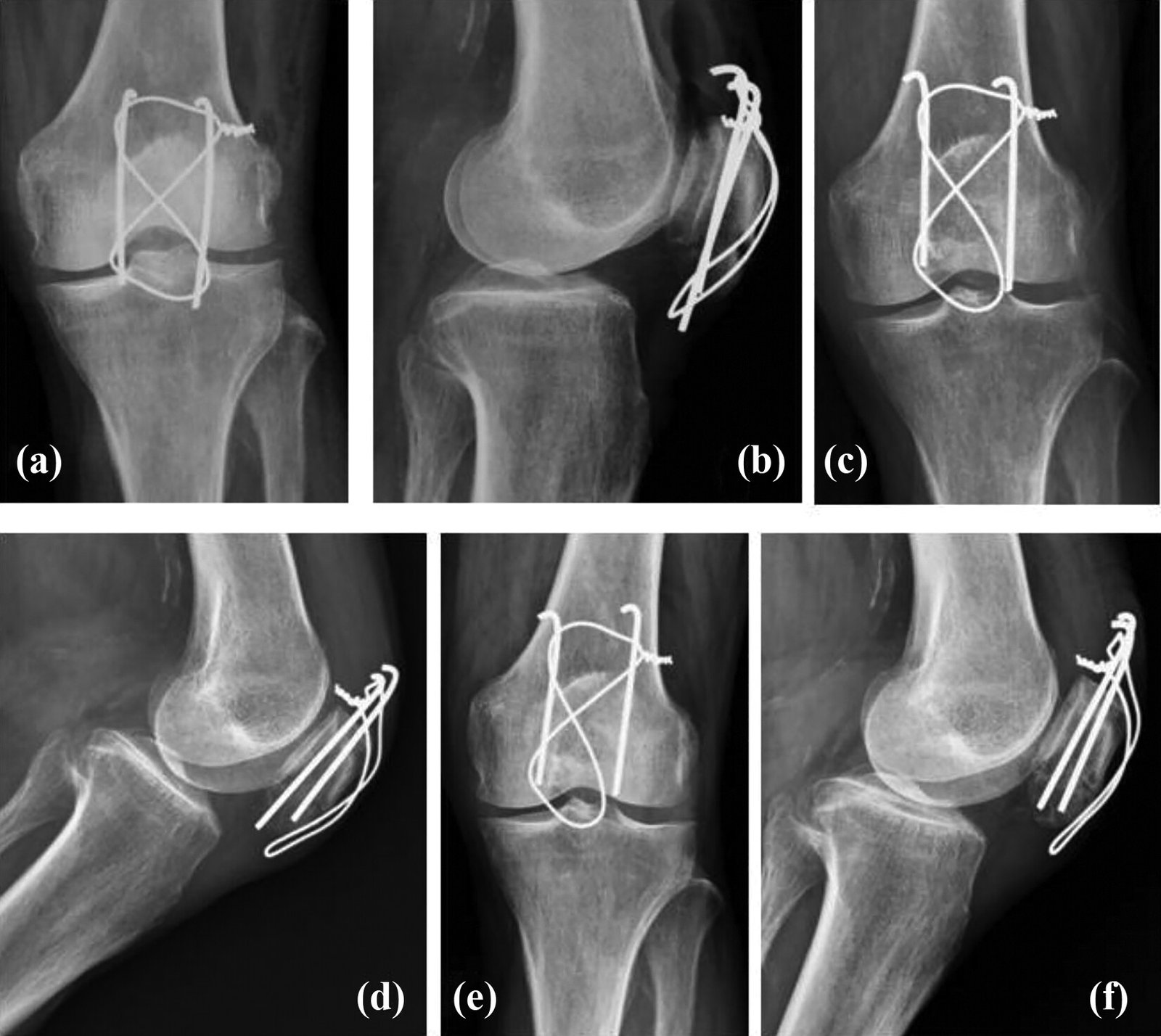
B) Displaced Fracture: In this variety, surgery is the treatment of choice. Surgery is performed as early as possible preferably within 7 days.
1) Open reduction and internal fixation.
2) Patellectomy.
3) Modified tension band wiring (MTBW) (2-K wires with anterior placement).
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-260-261]
Complications of fractures of patella:
A) Early complications:
1) Earl y fracture dehi scence.
2) Postoperative infection.
3) Refracture (15%).
4) Avascular necrosis (25% incidence in proximal pole).
B) Delayed complications:
1) Knee stiffness.
2) Osteoarthritis of the patellofemoral and knee joint extensor lag.
3) Delayed union.
4) Nonunion.
5) Loss of knee motion.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-262]
Disadvantages of patellectomy:
1) Strength of quadriceps returns slowly although knee motion is regained quite fast.
2) Obvious atrophy of the quadriceps muscle persists for months and often permanently.
3) Protection of the knee by the patella is lost.
4) Pathological ossification may develop where the patella is excised.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-262]