History Taking – Nursing is a profession within the healthcare sector focused on the care of individuals, families, and communities so they may attain, maintain, or recover optimal health and quality of life. Nurses may be differentiated from other healthcare providers by their approach to patient care, training, and scope of practice. Nurses practice in many specialisms with differing levels of prescriber authority.
Many nurses provide care within the ordering scope of physicians, and this traditional role has shaped the public image of nurses as care providers. However, nurses are permitted by most jurisdictions to practice independently in a variety of settings depending on training level. In the postwar period, nurse education has undergone a process of diversification towards advanced and specialized credentials, and many of the traditional regulations and provider roles are changing.
Nurses develop a plan of care, working collaboratively with physicians, therapists, the patient, the patient’s family, and other team members, that focus on treating illness to improve quality of life. Nurses may help coordinate the patient care performed by other members of an interdisciplinary healthcare team such as therapists, medical practitioners, and dietitians. Nurses provide care both interdependently, for example, with physicians, and independently as nursing professionals.
History Taking
Definition of Health History:
The health history is a current collection of organized information unique to an individual. Relevant aspects of the history include biographical, demographic, physical, mental, emotional, sociocultural, sexual, and spiritual data.
or
Health history is a chronological and detailed health record of the client. It is purpose is to elicit information regarding all the variable s that may affect the client’s health status.
Types of Health History
There are four types of health history such as-
A. Complete health history: It described in this text, is a comprehensive history of the patients past and present health status and converts many factors of a patient’s life.
B. Episodic health history: It is shorter and specific to the patients current reason for seeking health care,
- e.g.-The patients who seeks care for a sore throat and fever wound have an olen episodic health history,
C. Interval or follow up health history: It builds on a preceding visit to a health care facility. It documents the patient’s recovery from illness, such as the sore throat and fever or progress from a prior visit.
D. Emergency health history: It is elicited from the patient and other sources in an emergency situation. Only information required immediately to treat the emergent need for the patient is gathered; after the life threatening condition is no longer present, the nurse may elicit a more comprehensive history from the patient.
Purposes of Health History:
1. Perform physical assessment.
2. Review records- laboratory records, other health care records.
3. Interview supports persons.
4. Review literature.
5. Validate assessment data.
6. To identify the nursing needs of the patientiini
7. To establish a nursing diagnosis
8. To prepare a nursing care plan.
9. To give complete nursing intervention.
10. To evaluate the effectiveness of nursing interventions.
Requirement of Good Communication Skills for History Taking:
. To establish and maintain a relationship with patients and their families.
2. To encourage patients to describe all relevant aspects of their problems.
3. To get and give accurate information.
4. To use time and opportunity effectively.
5. To improve patient satisfaction with the care given.
6. To improve thrust and cooperation with the care.
7. To reduce negative emotions and fear.
Information Will Maintain to Sequence of Categories for Health History
The health history is adapted to include information specific for age and development stage of the person. Nurses have to focus on different information according to age and the development stage of each individual.
- Biological data and source of history.
- Reason for seeking care.
- Present health history or present illness.
- Past history.
- Family history.
- Review of systems.
- Functional assessment or activity of daily living.
Tips for Obtaining a Meaningful History:
1. The quality of a history improves with experience with the interviewing process. Tips for obtaining a meaningful history include:
2. Be a good listener.
3. Listen carefully and attentively for whole thoughts and ideas, not merely isolated facts.
4. Use skills of active listening, silence and acceptance to provide ample time for the person. Be as objective as possible.
5. Identify only the clients and/or significant others contribution to the history.
Framework/Format of a Patient Assessment Form:
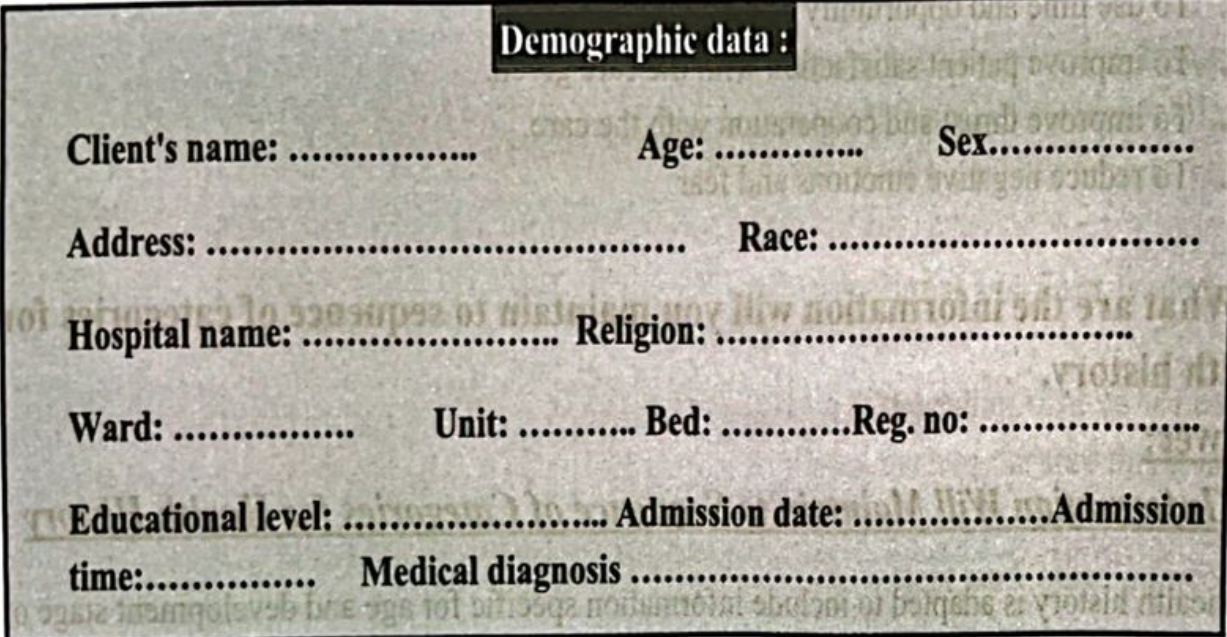
Data Collection:
A. Health history:
a) Chief complain:………………………………………………………………………………………..
b) History of Present illness:………………………………………………………………………..
c) History of past illness:………………………………………………………………………………..
B. Family history :………………………………………………………………………………………..
C. Physical examination:………………………………………………………………..
a) General appearance………………………………………………………………….
b) Temperature:……………………………………………………………………………..
c) Pulse:……………………………………………………………………………………………..
d) Respiration:………………………………………………………………………………
e) BP :……………………………………………………………………………………. mmHg
1) Height…………………………………………………………………………………
g) Weight:……………………………………………………………………..
D. Health pattern assessment:
a) Health perception – health management pattern ………………………………………………………………………………
b) Nutritional metabolic pattern :…………………………………………………………………………………………………………..
c) Pattern of elimination:………………………………………………………………………………………………….
d) Pattern of activity & exercise:……………………………………..
e) Cognitive perceptual pattern:…………………………………………………….
f) Pattern of sleep & rest:……………………………………………………………………..
g) Pattern of self perception & self concept:…………………………………………………………………..
h) Role relationship pattern:…………………………………………………………………….
i) Sexual reproductive pattern ……………………………………………………………………….
j) Pattern of coping & stress tolerance:…………………………………………………………………..
k) Pattern of values & beliefs……………………………………………………………………….
E. Sign and symptoms during care of the patient:………………………………………………………………………
F. Treatment during taking care of the patient:………………………………………………………………………
G. Laboratory and investigation: ………………………………………………………………………

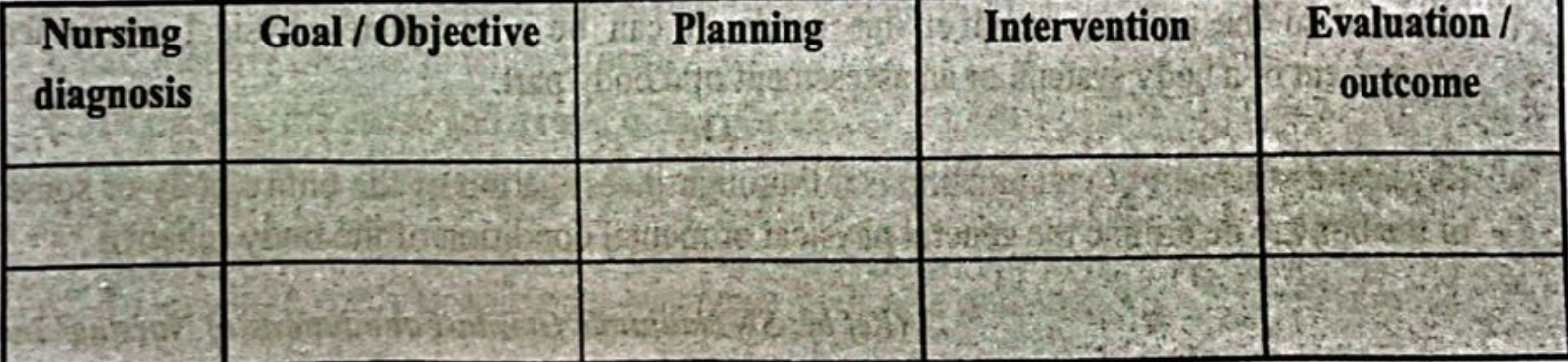
H. Nursing Care Plan:
Components of Health History
1. Particulars of patient.
2. Presenting/chief complaints.
3. History of present illness.
4. History of past illness.
5. Drug history.
6. Family history.
7. Personal & social history.
8. Occupational history.
9. Immunization history.
10. Menstrual history (in case female).
11. General examination.
12. Systemic examination.
13. Salient features.
14. Provisional diagnosis.
15. Differential diagnosis.
16. Investigations.
17. Confirmed diagnosis.
18. Treatment.
19. Follow up.