HIV and AIDS – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
HIV and AIDS
Acquired immune deficiency syndrome (AIDS):
AIDS, the acquired immune deficiency syndrome is a end stage of Human immune deficiency viral infection which breaks down the body’s immune system, leaving the victim vulnerable to a host of life threatening opportunistic infections, neurological disorders or unusual malignancy.
Causative organism:
HIV Human Immunodeficiency syndrome
Incubation period: 6 months to 6 years
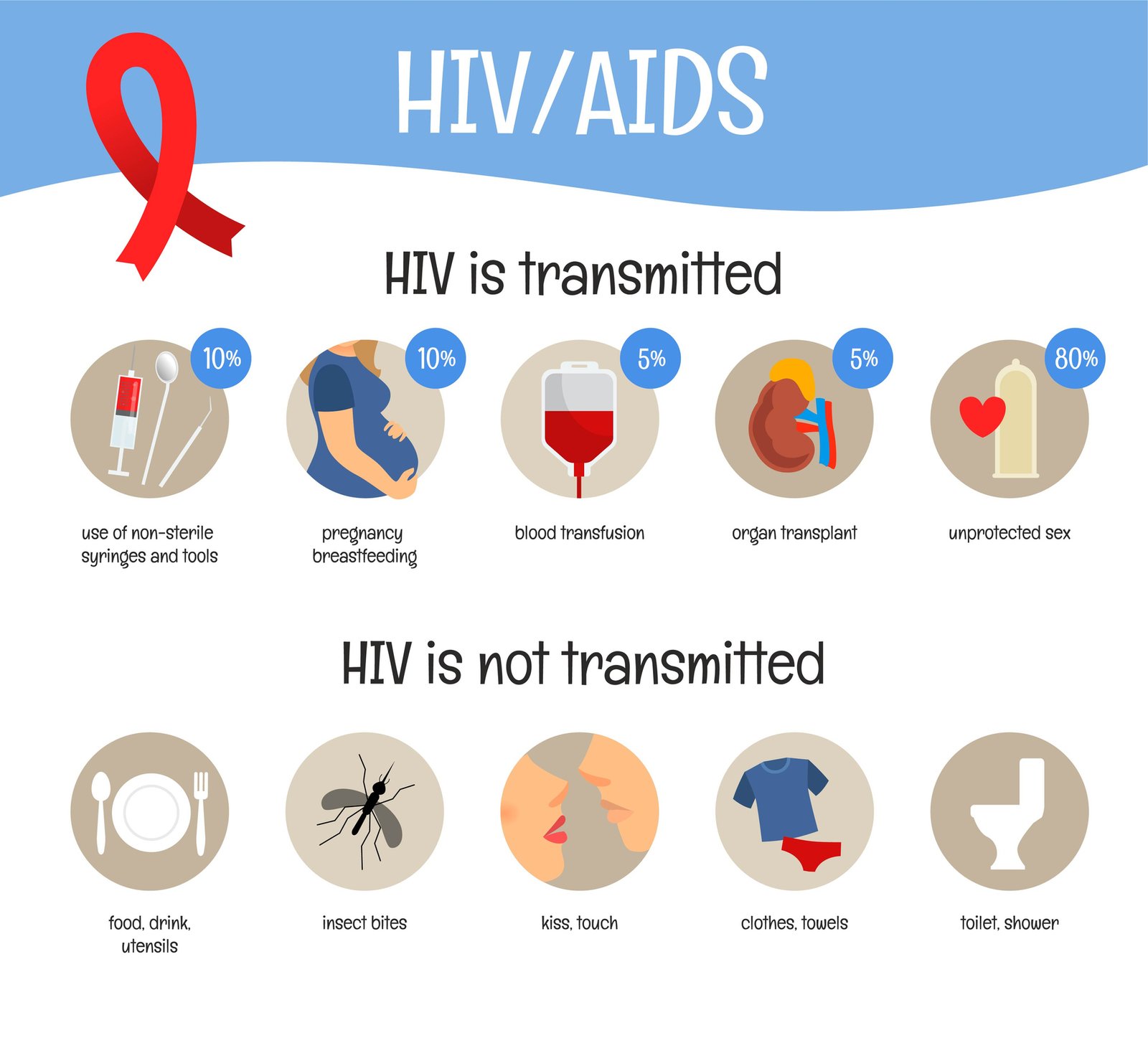
Route of transmission:
- Sexual transmission.
- Contaminated blood & blood products.
- Maternal to fetal through – placenta & breast feeding.
Mode of transmissions:
- Sexual intercourse (anal and vaginal).
- Intravenous drug users.
- Transmission of contaminated blood or blood products
- Use of contaminated needles, needle stick injuries
- Mother to child by breast feeding.
- Perinatal transmission.
Diagnosis:
Clinical presentations:
1. Asymptomatic.
2. Active infection syndrome is characterized by:
- Diarrhoea
- Fever
- Rash
- Arthralgia
- Lympadenopathy
3. AIDS-related complex:
- Fever
- Weight loss
- Diarrhoea
- Skin rash
- Lymphadenopath
- Herpes simplex.
- Oral candidiasis.
- Oral or genital ulcers.
- PID.
- Tubo-ovarian mass.
- Thrombocytopenia
Investigations:
- Detection of anti-HIV antibody in serum.
- Acute infection may be detected by the presence of P24 antigen or HIV RNA by PCR and precedes the appearance of IgM and IgG (within 3 months).
- During the asymptomatic period there are high titres of IgG to core and envelope proteins.
- As immunodeficiency develops, IgG titre to core protein falls, and P24 antiginaemia recurs.
- ELISA test: Demonstration of serum antibody to HIV.
- Western blot test (immunoblot).
- HIV-RNA.
- Polymerase chain reaction(PCR): It is gold standard for diagnosis of HIV
Treatment:
1. Anti-retroviral therapy:
Nucleoside Reverse Transriptase Inhibitors (NRTIs):
- Zidovudine.
- Lamivudine.
Non- Nucleoside Reverse Transcripase Inhibitors (NNRTIs):
- Delviridine.
- Nevirapine.
- Efavirenz.
Protease inhibitors:
- Indinavir
- Saquinavir.
- Ritonavir.
Fusion inhibitor:
- Enfuviritide.
2. Drus combinations:
- Two fromNRTIs + one fromNNRTIs.
- Two from NRTIs + one from protease inhibitors
Prevention:
- Health & sex education.
- Prevention of blood born STDs transmission.
- Control of prostitution.
- Social welfare measures..
- Abiding by the law of religion.
- Early diagnosis & treatment.
- Post-exposure prophylaxis with Zidovudine & lamivudine is advisable.
- Terminltion of pregnancy in HIV positive women.
- Avoiding breastfeeding.
- Wide spread voluntary counseling & testing (VCT).
Vertical transmission of AIDS:
The transmission of AIDS to the neonates from the infected mother is about 14-25%. The baby may be affected in utero through transplacental transfer, during delivery by contaminated… secretions and blood of the birth canal and through breast milk
Process of vertical transmission:
1. Transplacental transfer.
2. During delivery by contaminated secretions
3. Blood of the birth canal..
4. Through breast milk in neonatal period.
Prevention of vertical transfer:
5. Routine anfenatal HIV antibody testing.
6. Counselling about risks of pregnancy if HIV seropositive’
7. Measures to reduce vertical trinsmission
- Highly active antiretroviral therapy (FIAART) treatment düring pregnancy.
- Perinatalantiretroviralprophylaxis.
- Caesarean section.
Condvloma accuminata:
These are common multiple vulval warts. They are small papules that are sometimes sessile and often polypoid. They are coarse, flat-topped, moist & necrotic.
Cause: Infection by human papilloma virus.
Risk factors:
- Multiple sexual partners.
- Presence of viganal infections- candidiasis, trichomoniasis or bacterial vaginosis.
C/F:
- Asymptomatic.
- Painless, raised, soft, fleshy, growths on the vulva, vagina, cervix urethral meatus, perineum and anus.
- Abnormal cervical cytologic changes common.
Investigation: Colposcopy& biopsy
Treatment:
1. Cytolytic topical agents:
- Trichloroacetic acid.
- Podophyllin.
2. Physical ablative methods:
- Laser
- Cryotherapy
- Electrodesiccation.
3. In rarely selected cases- surgical excision or tangential shaving may be used.
Long term complications of Chlamydia trachomatis infections:
- Urethritis &bartholinitis.
- Salpingitis causes tubal scarring resulting in infertility and ectopic pregnancy.
Thyroid disorders
Concept of thvroid disorder:
Thyroid disease is common in women of reproductive age. The incidence of thyroid disease associated with pregnancy is varied. Hyperthyroidism occurs, in about two per 1,000 pregnancies and hypothyroidism about nine per 1,000 (girling, 1996).
Thyroid disease in pregnancy can have potential adverse effects on the fetus; the fetal morbidity and mortality rates in untreated women can be as high as 50 percent (sugrue and drury, 1980).