Medical Definition of Pneumonia – This course is designed to understand the concept of community health nursing: nurses’ roles and interventions in family health, school health, occupational health, environmental health, elderly health care, gender issues, disaster management and principles and terminology of epidemiology. The aim of the course is to acquire knowledge and skills in community health nursing.
Medical Definition of Pneumonia
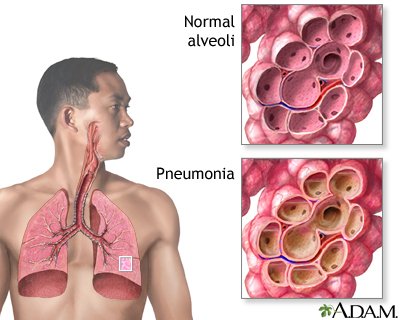
Pneu-monia is an infection that inflames the air sacs in one or both lungs. The air sacs may fill with fluid or pus (purulent material), causing cough with phlegm or pus, fever, chills, and difficulty breathing. A variety of organisms, including bacteria, viruses and fungi, can cause pneu-monia.

Pneu-monia can range in seriousness from mild to life-threatening. It is most serious for infants and young children, people older than age 65, and people with health problems or weakened immune systems.
Definition of Pneumonia
Pneu-monia can be defined as any infection in the lungs parenchyma.
Or,
Pneu-monia can be defined as an acute respiratory illness associated with recently developed radiological pulmonary shadowing which may be segmental lobar or multi-lobar.
Or,
Pneumonia is an infection that inflames the air sacs in one or both lungs. The air sacs may fill with fluid or pus (purulent material), causing cough with phlegm or pus, fever, chills, and difficulty breathing.
(Ref by-Davidsons Medicine/224/682)
Classification/Causes of Pneumonia
A. Anatomical, clinical and radiographic presentation.
a) Lobar pneumonia: consolidation of a large portion or entire lobe of lung.
b) Bronchopneumonia: Patchy consolidation in lung. atypical pneumonia
B. Clinical classification:-
a) Community acquired pneumonia-
b) Hospital acquired pneumonia
c) Pneumonia in immune-compromised hosts
d) Pneumonia in damaged lung
C. Aetiological classification:
1) Infective
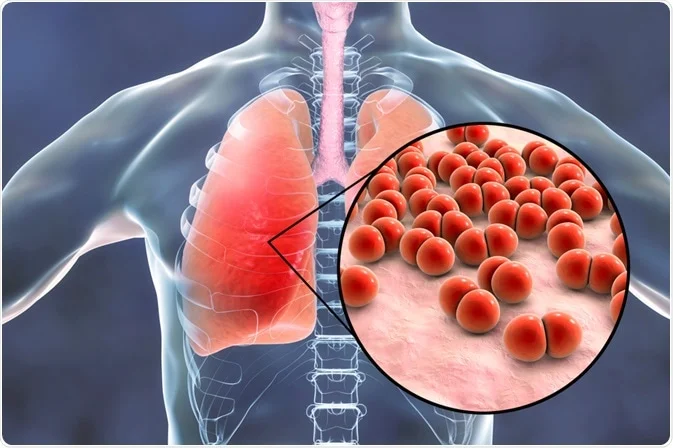
a) Bacterial
- Pneumoccoci
- Staphylococcus aureus
- Streptococcus pyogens
- Haemophilus Influenza
- Mycoplasma pneumoneae
- Klebsiella Pneumonia
- M. Tuberculosis
b) Viral
Respiratory syncytial virus
- Influenza and Para influenza
- Cytomegalo virus
- Measles virus
- Mumps virus
- Rhino virus
- Adeno virus
c) Fungal: Candida, Actinomycosis, and Histoplasma.
d) Protozoal: E. histolytica, Toxoplasma gondii, Pneumocystitis carinii.
e) Mycoplasmal: M. Pneumonia
f) Chlamydial: C. Psittaci
g) Ridkettsial: Typhus and Q-fever,
2) Allergic: Collagen vascular disease
3) Chemical agents: fumes, gas
4) Physical: Irradiation
D. Clinical classification of pediatrics:
a) 2 month to 5 years
- very severe disease
- severe pneumonia
- pneumonia
- No pneumonia: Cough and cold
b) Less than 2 month
- very severe disease
- severe pneumonia
- No pneumonia: Cough and Col
(Ref by-Davidsons Medicine/224/683)
Diagnosis of Pneumonia
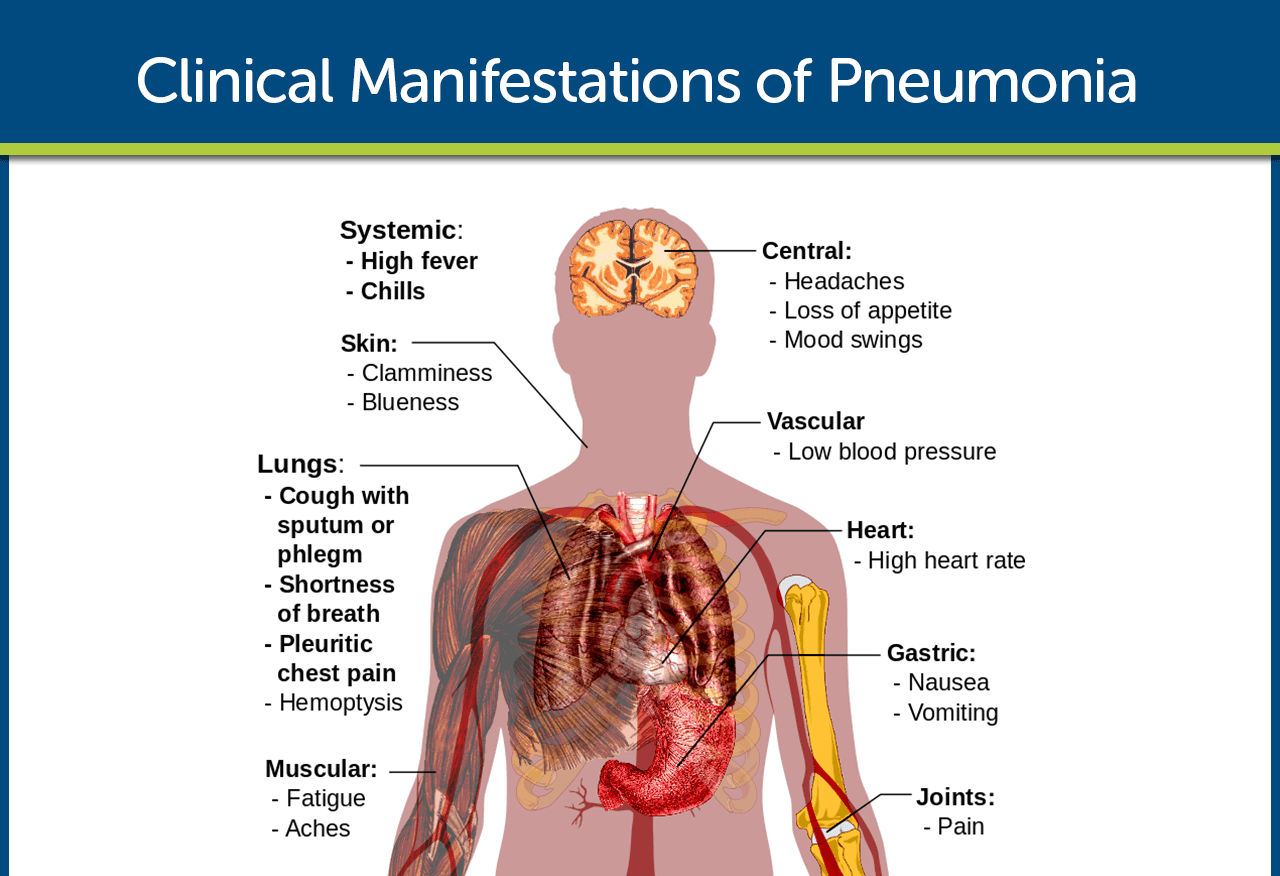
A. Symptoms
a) Fever
- Sudden onset
- High fever
- Usually associated with rigor & vomiting.
b) Chest pain
- Pleuritic chest pain.
- Occasionally referred to the shoulder or anterior abdominal wall.
c) Cough
- Short, painful.
- At first dry.
- Later become productive and may become rust coloured or even frankly blood stain
d) Dyspnoea
e) Loss of appetite & headache
B. Signs
a) Tachycardia,,
b) Pyrexia,
c) Tachypnea,
d) Cyanosis,
e) Hypotension,
1) Confusion
C. Routine examination (R/E)
a) Inspection
- Respiratory rate in increased
- Respiratory movement is diminished on the affected side
b) Palpation
- Trachea-central, may be shifted to the opposite side (in pleural effusion)
- Apex beat-normal in position, may be shifted to the opposite site
- Chest walls movement is diminished on the affected side
c) Percussion
- Woody dull in case of consolidation
- Stony dull in case of pleural effusion
d) Auscultation
- Breath sound is high pitched bronchial in consolidation and diminished
- Vocal resonance is increased in consolidation and diminished or absent in pleural effusion.
- Fine crepitation early and coarse crepitation in resolution phase
D. Investigation
a) Blood: TC, DC, ESR, and culture sensitivity test.
b) Sputum
- Gram stain-Gram positive diplococci
- culture and sensitivity-pneumococcus can be isolated
c) Chest X-ray test
d) Serological test – To detect the pneumococcal antigen.
(Ref by- Kumar & Clark clinical Medicine /7 +Harrison’s internal medicine/17+ short case Abdullah Sir 4 +Davidson’s Medicine 683-85/22)
Management of Pneumonia
1. Rest in bed.
2. O, inhalation if necessary/Difficulty in breathing
3. Adequate hydration by fluid balance-I/V if only severe cases otherwise normal.
4. Antibiotic-depends on severity & type
5. Treatment for Community Acquired pneumonia (CAP):
A. Uncomplicated CAP:
a) Amoxicillin 500 mg 8-hourly orally
b) If patient is allergic to penicillin
- Clarithromycin 500 mg 12-hourly or
- Erythromycin 500 mg 6-hourly orally
c) If Staphylococcus is cultured or suspected
- Flucloxacillin 1-2 g 6-hourly i.v. plus
- Clarithromycin 500 mg 12-hourly i.v.
d) If Mycoplasma or Legionella is suspected
- Clarithromycin 500 mg 12-hourly orally or iv. or
- Erythromycin 500 mg 6-hourly orally or i.v. plus
- Rifampicin 600 mg 12-hourly i.v. in severe cases
B. Severe CAP
a) Clarithromycin 500 mg 12-hourly i.v. or
b) Erythromycin 500 mg 6-hourly i.v. plus
c) Co-amoxiclav 1.2 g 8-hourly i.v. or
d) Ceftriaxone 1-2 g daily i.v. or
e) Cefuroxime 1.5 g 8-hourly i.v. or
f) Amoxicillin 1 g 6-hourly i.v. plus flucloxacillin 2 g 6-hourly i.v.
6. Hospital acquired pneumonia:
a) Cefotaxime plus gentamycin or
b) Meropenem
7. Aspiration pneumonia:
a) Co-amxiclav 1.2 gm 8 hourly plus Metronidazole 500 mg 8 hourly.
8. Treatment of pleural pain-Opiates such
b) Pathedine 50-100 mg or Morphine 10 mg IM or IV.
(Ref by-Kumar & Clark clinical Medicine /7th +Harrison’s internal medicine/17th + short case Abdullah Sir +Davidson’s Medicine 683-85/224)
Nursing Management of Pneumonia
A. To improve airway patency
a) Removal of secretions. Secretions should be removed because retained secretions interfere with gas exchange and may slow recovery.
b) Adequate hydration of 2 to 3 liters per day thins and loosens pulmonary secretions.
c) Humidification may loosen secretions and improve ventilation.
d) Coughing exercises. An effective, directed cough can also improve airway patency.
e) Chest physiotherapy. Chest physiotherapy is important because it loosens and mobilizes secretions.
B. To promote rest and conserve energy
a) Encourage avoidance of overexertion and possible exacerbation of symptoms.
b) Semi-Fowler’s position. The patient should assume a comfortable position to promote rest and breathing and should change positions frequently to enhance secretion clearance and pulmonary ventilation and perfusion.
C. To promote fluid intake
a) Fluid intake. Increase in fluid intake to at least 21. per day to replace insensible fluid losses.
D. To maintain nutrition
a) Fluids with electrolytes. This may help provide fluid, calories, and electrolytes.
b) Nutrition-enriched beverages. Nutritionally enhanced drinks and shakes can also help restore proper nutrition.
E. To promote patient’s knowledge
a) Instruct patient and family about the cause of pneumonia, management of symptoms, signs, and symptoms, and the need for follow-up.
b) Instruct patient about the factors that may have contributed to the development of the disease.
Factors That Predispose to Pneumonia
1. Upper respiratory tract infection
2. Alcohol
3. cigarette smoking
4. corticosteroid therapy
5. Old age
6. recent influenza infection.
7. indoor air pollution
8. AIDS
9. preexisting lungs disease
(Ref by-Davidsons Medicine/224/682)
Pathophysiological Condition of Pneumonia
Having an idea about the disease process helps the patient understand the treatment regimen and its importance, increasing patient compliance.
A. Pneumonia arises from normal flora present in patients whose resistance has been altered or from aspiration of flora present in the oropharynx.
B. An inflammatory reaction may occur in the alveoli, producing exudates that interfere with the diffusion of oxygen and carbon dioxide.
C. White blood cells also migrate into the alveoli and fill the normally air-filled spaces.
D. Due to secretions and mucosal edema, there are areas of the lung that are not adequately ventilated and cause partial occlusion of the alveoli or bronchi.
E. Hypoventilation may follow, causing ventilation-perfusion mismatch.
F. Venous blood entering the pulmonary circulation passes through the under ventilated areas and travels to the left side of the heart deoxygenated.
G. The mixing of oxygenated and poorly oxygenated blood can result to arterial hypoxemia.
Complications of Pneumonia
Even with treatment, some people with pneumonia, especially those in high-risk groups, may experience complications, including:
1. Bacteria in the bloodstream (bacteremia). Bacteria that enter the bloodstream from your lungs can spread the infection to other organs, potentially causing organ failure.
2. Difficulty breathing.
3. Fluid accumulation around the lungs (pleural effusion).
4. Lung abscess.