Medical Umbilical cord – The course is designed for the basic understanding of anatomical structures and physiological functions of human body, musculoskeletal system, digestive system, respiratory system; cardiovascular system; urinary system, endocrine system, reproductive system, nervous system, hematologic system, sensory organs, integumentary system, and immune system.The aim of the course is to acquire knowledge and skills regarding anatomy and physiology.
Medical Umbilical cord
The umbilical cord or funis forms the connecting link between the fetus and the placenta through which the fetal blood flows to and from the placenta. It extends from the fetal umbilicus to the fetal surface of the placenta.

DEVELOPMENT:
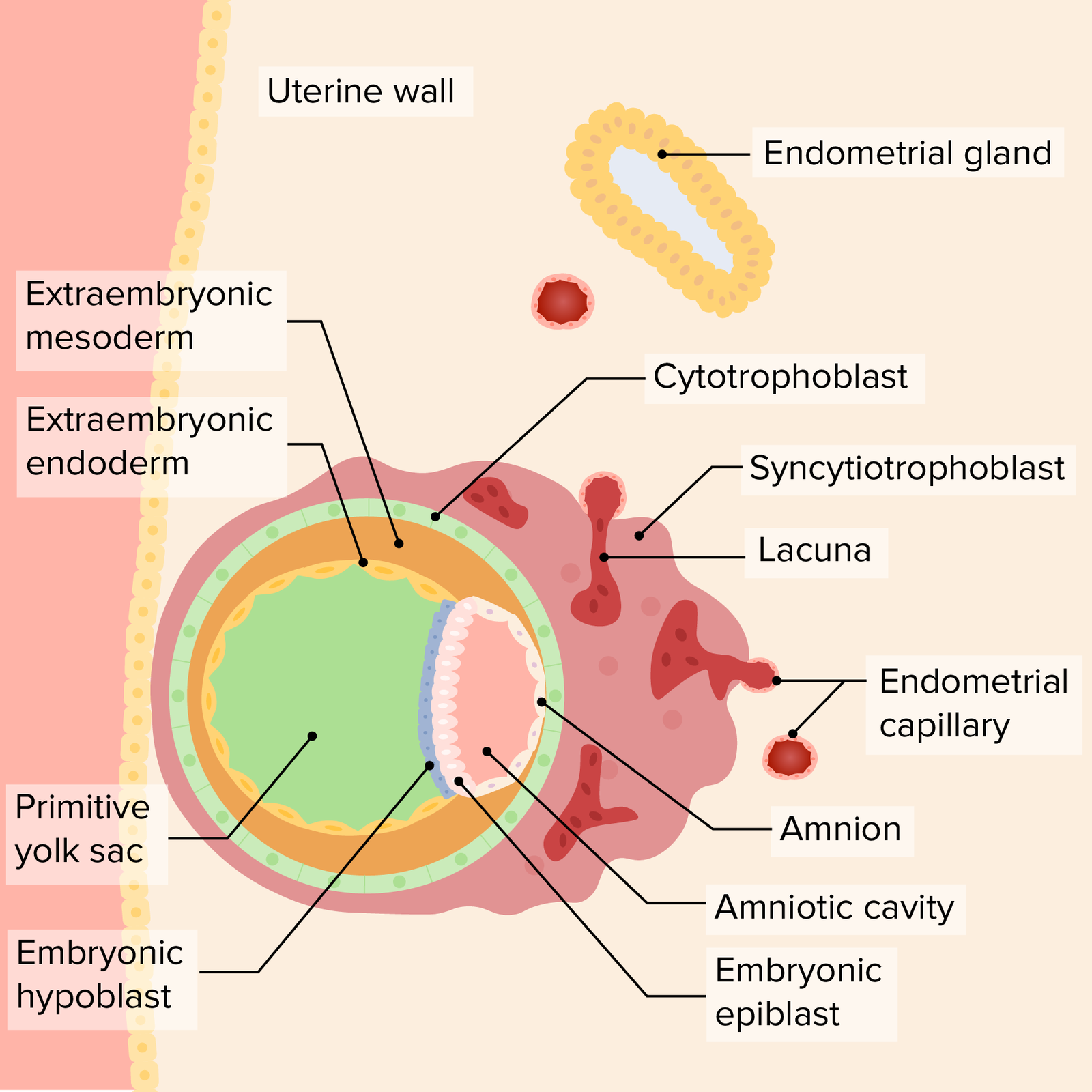
The umbilical cord is developed from the connective stalk or body stalk, which is a band of mesoblastic tissue stretching between the embryonic disc and the chorion. Initially, it is attached to the caudal end of the embryonic disc but as a result of cephalocaudal folding of the embryo and simultaneous enlargement of the amniotic cavity, the amnioectodermal junction converges on the ventral aspect of the fetus.
As the amniotic cavity enlarges out of proportion to the embryo and becomes distended with fluid, the embryo is carried more and more into the amniotic cavity with simultaneous elongation of the connective stalk, the future umbilical cord.
(Ref: DC Dutta’s Textbook of Obstetrics, 7th edition)
STRUCTURES:
The constituents of the umbilical cord when fully formed are as follows
1. Covering epithelium: It is lined by a single layer of amniotic epithelium but shows stratification like that of fetal epidermis at term.
2. Wharton’s jelly:It consists of elongated cells in a gelatinous fluid formed by mucoid degeneration of the extraembryonic mesodermal cells. It is rich in mucopolysaccharides and has got protective function to the umbilical vessels.
3. Blood vessels: Initially, there are four vessels two arteries and two veins. The arteries are derived from the internal iliac arteries of the fetus and carry the venous blood from the fetus to the placenta. Of the two umbilical veins, the right one disappears by the 4th month, leaving behind one vein which carries oxygenated blood from the placenta to the fetus. Presence of a single umbilical artery is often associated with fetal congenital abnormalities (see p. 218)
4. Remnant of the umbilical vesicle (yolk sac) and its vitelline duct: Remnant of the yolk sac may be found as a small yellow body near the attachment of the cord to the placenta or on rare occasion, the proximal part of the duct persists as Meckel’s diverticulum.
5. Allantois: A blind tubular structure may be occasionally present near the fetal end which is continuous inside the fetus with its urachus and bladder.
6. Obliterated extraembryonic coelom: In the early period, intraembryonic coelom is continuous with extraembryonic coelom along with herniation of coils of intestine (midgut). The condition may persist as congenital umbilical hernia or exomphalos
CHARACTERISTICS:
It is about 40 cm in length with an usual variation of 30-100 cm. Its diameter is of average 1.5 cm with variation of 1-2.5 cm. Its thickness is not uniform but presents nodes or swelling at places. These swellings(false knots) may be due to kinking of the umbilical vessels or local collection of Wharton’s jelly.
True knots (1%) are rare. Long cord may form loop around the neck (20-30%). It shows a spiral twist from the left to right from as early as 12th week due to spiral turn taken by the vessels-vein around the arteries. The umbilical arteries do not possess an internal elastic lamina but have got well developed muscular coat. These help in effective closure of the arteries due to reflex spasm soon after the birth of the baby. Both the arteries and the vein do not possess vasa vasorum.
ATTACHMENT:
In the early period, the cord is attached to the ventral surface of the embryo close to the caudal extremity but as the coelom closes and the yolk sac atrophies, the point of attachment is moved permanently to the center of the abdomen at fourth month. Unlike the fetal attachment, the placental attachment is inconsistent.
It usually attaches to the fetal surface of the placenta somewhere between the center and the edge of the placenta-calledeccentric insertion. The attachment may becentral, marginal or even on the chorion laeve at a varying distance away from the margin of the placenta, calledvelamentous insertion
(Ref: DC Dutta’s Textbook of Obstetrics, 7th edition, 2013)