
Plasmodium falciparum, vivax, ovale, malariae (Malaria) – Basic microbiology, parasitology, and immunology; nature, reproduction, growth, and transmission of common microorganisms and parasites in Bangladesh; prevention including universal precaution and immunization, control, sterilization, and disinfection; and specimen collections and examination. Students will have an understanding of common organisms and parasites caused human diseases and acquire knowledge about the prevention and control of those organisms.
Plasmodium falciparum, vivax, ovale, malariae (Malaria)
Definition of Malaria:
Malaria is an infectious disease caused by plasmodium and transmitted by the bite of female anopheles mosquito, characterized by-fever, anemia, splenomegaly etc.
or
Malaria is a protozoal disease caused by infection with parasites of the genus plasmodium and transmitted to man by certain of infected female anopheles mosquito.
Epidemiological Features of Malaria:
A) Agent factors:
a) Agent: Malaria in man is caused by 4 distinct species of malaria parasite
- Plasmodium vivax
- Plasmodium falciparum.
- Plasmodium malariae
- Plasmodium ovale
b) Reservoir of infection: Human
c) Period of communicability: Malaria is communicable as long as gametocytes exist in lanin the blood to infect vector mosquito,
B) Host factors:
a) Age: Malaria affects all ages
b) Sex: Male are more exposed than female
c) Social and economic factor: More in underdeveloped countries
d) Housing: More in all ventilated and ill lighted house
e) Pregnancy: The risk
f) Occupation: More in agriculture practitioner
g) Human habits sleeping out of house and mosquito net
C) Environmental factors:
a) Season: Maximum prevalence is from July to November
b) Temperatures: 20°C -30°C
c) Humidity: 60%
d) Rain fall: Necessary for breeding
D) Mode of transmission:
a) Vector transmission: Infected female anopheles mosquito
b) Direct transmission:
- Blood transmission
- Infected needles
- Congenital-very very rare
E) Incubation period: Varies according to species –
a) 12 (9-14) days for P. falciparum
b) 14 (8-17) days for P. vivax
c) 28 (18-40) days for P. malariae
d) 17 (16-18) days for P. ovale
Classification of Plasmodium/Malarial parasites;
1. Plasmodium vivax
2. Plasmodium falciparum
3. Plasmodium ovale
4. Plasmodium malariae

The species of malarial parasites found in Bangladesh.
The following 2 species of plasmodium are more common in Bangladesh –
1. Plasmodium vivax: common in plain land.
2. Plasmodium falciparum: common in hilly areas.
Clinical Types of Malaria and the Causative Plasmodium Parasites:
| Clinical types of malaria | Plasmodium parasite |
| 1. Benign tertian malaria |
|
| 2. Malignant tertian malaria | Plasmodium falciparum |
| 3. Quartan malaria | Plasmodium malariae |
Difference between P. Vivax & P. Falciparum:
| Traits | P. vivax | falciparum |
| Schizogony | 48 hours | 48 hours or under |
| Forms in peripheral blood | Trophozoites, schizonts and gametocytes. | Rings and crescents only. |
Trophozoites- a) Ring form b) Growing form | Size, 2.5 micrometer; cytoplasm is thicker. | Size, 1.25 to 1.5 micrometer, cytoplasm is thinner. |
| Irregular with a vacuole. | Assumes a compact form. | |
| Schizont (mature) | Size, 9 to 10 micrometer, regular. | Size, 4.5 to 5 micrometer. Fill two-thirds of a R.B.C. |
| Merozoites | 12 to 24, arranged in irregular grape-like cluster | 18 to 24 or more, arranged in a grape-like cluster |
| Malarial pigments | Yellowish-brown, fine granules | Dark-brown or blackish. |
| Infected R.B.C | Enlarged, pale, Schuffher’s dots present. | Usually unaltered, crenation, reddish violet colour and Maurer’s dots. |
| Gametocyte | Spherical | Crescentic (banana-shaped). |
Dangerous Malaria;
- Falciparum malaria is dangerous as
- They can infect both mature & immature RBC (reticulocytes). So, there is severe anaemia. On the other hand, other malaria species only infect immature RBC (reticulocyte).
- Falciparum shows resistance to common antimalarial drugs.
- Complications are higher and fatal, e.g. – cerebral malaria, black water fever etc.
- Early diagnosis is difficult, so patient rapidly developed complications
Life Cycle of Malarial Parasites:
➤ Human cycle / asexual cycle. –
➤ Mosquito cycle / sexual cycle.
Human cycle (Asexual cycle): 4 stages
1. Pre-erythrocytic schizogony / hepatic schizogony; Mosquito bite → Sporozoites injected to host → spreads to surrounding tissue → Peripheral circulation → Enter into liver parenchyma → Sporozoites become schizonts → Rupture of schizonts → Liberation of merozoites →
- Micromerozoites → Enter into circulation.
- Macromerozoites → Re-enter into liver cells
2. Erythrocytic schizogony; Micromerozoite enters into RBC→ Trophozoites → Schizont → t Rupture of schizonts → Liberation of merozoite→ Attacks healthy RBC→ Cycle is repeated.
This phage is responsible for clinical attack of malaria
3. Gametogony: Some merozoites inside the RBC of capillaries of internal organs (spleen, bone marrow) develop into gametes Peripheral blood.
4. Exo-erythrocytic schizogony: Except P. falciparum, in other species of Plasmodium, there is exo- erythrocytic schizogony. Because the tissue phage persists in the form of merozoites life cycle, parasite remains dormant of potentially infective to give rise infection to time (relapse)
Mosquito cycle (sexual cycle):
Female anopheles mosquito Blood mealMacrogametocytes and microgametocytes are taken up Fertilization of macrogametes (round) by microgametes (long) Fertilized macrogamete (ookinete) in intestinal wall of mosquito Oocyst Meiotic & mitotic division → Sporozoites (100-1000) within Oocyst Rupture of Oocyst Release of sporozoites in the body cavity Through the circulation, the sporozoites are distributed to various organs & tissues, specially salivary gland & duct Bite Infection..
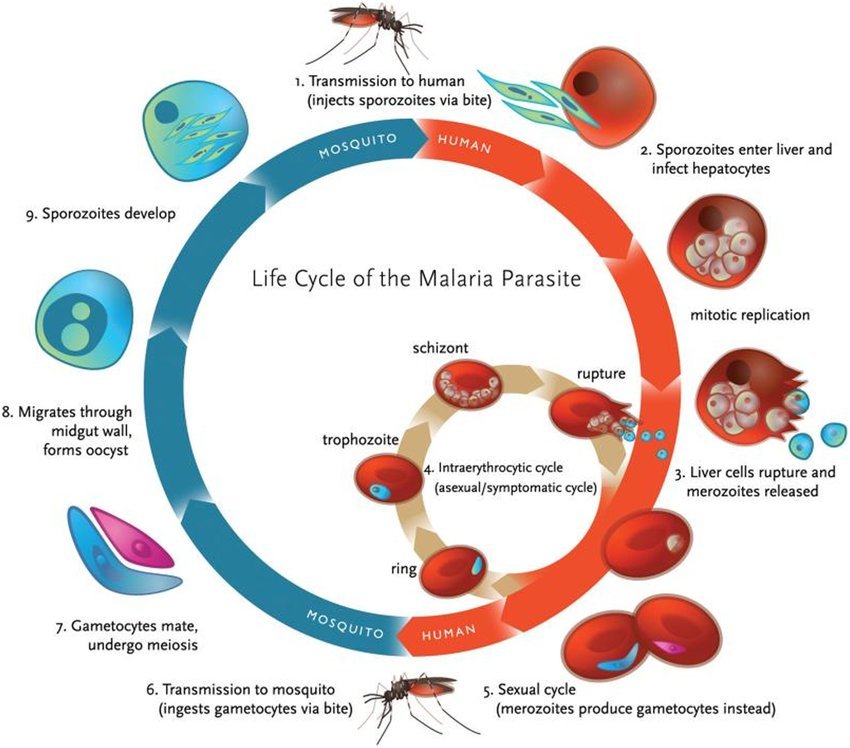
Figure: Life cycle of malaria parasite
why malaria cannot be eradicated from Bangladesh?
The factors those are responsible for difficulties of malaria eradication programme in Bangladesh are –
a. Administrative failure:
- Shortage of finance, manpower, drugs, insecticides transport
- Shortage of administrative personnel’s
b. Technical failure: Development of insecticides in vector and parasitic resistance to to drugs
c. Operational failure: Due to inadequate surveillance, case detection and treatment
d. General failure:
- Common border of Bangladesh and India
- Sleeping without mosquito net
- Poor standard of environmental sanitation
- Lack of health education
e. Epidemiological factors:
- Presence of extra-lumax reservoir of infection
- Presence of human carrier state
- Presence of sub clinical cases
The laboratory diagnosis of malaria.
History:
a) Patient may give H/O travel of malarious locality
b) Onset is insidious with malaise, headache, vomiting
c) Fever:
- No particular pattern
- Cold, hot and sweating stages are seldom found
- Not so high temperatures
d) Cough and mild diarrhea
e) Weakness
f) Patient may present with complication of the disease
- Unconsciousness
- Acute renal failure
- Black water fever
- Acute renal respiratory syndrome
- Septicemia
On examination (O/E):
- Patient anemia
- Jaundice may present
- Increase Temperature
- Hepato splenomegaly
Lab. diagnosis of malaria:
A) Direct evidences
- Thick film: To detect the presence of parasite
- Thin film: To detect the species of parasite
B) Indirect evidences:
- Serological test
- Blood for TC, DC, ESR, Hb%
- Liver function test
- Examination of urine
Signs Symptoms of Malaria:
1. Paroxysms with shaking chills
2. Rapidly rising fever with severe headache
3. Profuse sweating
4. Myalgia, with feeling of well-being in between
5. Splenomegaly, hepatomegaly
6. Orthostatic hypotension
7. Paroxysms may last for 12 hours, then, maybe repeated daily or after a day or two.
8. In children:
- Fever maybe continuous
- Convulsions and gastrointestinal symptoms are prominent
- Splenomegaly
9. In cerebral malaria
- Changes in sensorium, severe headache, and vomiting
- Jacksonian or grand mal seizure may occur
Mode of Transmission:
1. Vector transmission: Infected female anopheles mosquito
2. Direct transmission:
- Blood transmission
- Infected needles
- Congenital-very very rare
3. Incubation period: Varies according to species –
- 12 (9-14) days for P. falciparum
- 14 (817) days for P. vivax
- 28 (18-40) days for P. malariae
Complications of Malaria
➤ Pernicious malaria: 3 types-
- Cerebral
- Algid
- Septicaemic
➤ Black-water fever due to intra-vascular haemolysis.
➤ Hypoglycaemia especially with quinine treatment.
➤ Lactic acidosis.
➤ Prolonged hyperthermia
➤ Shock – Hypotensive or secondary to septicaemia.
➤ Pulmonary, cardiac, hepatic or renal dysfunction
➤ Seizures.
➤ Spontaneous bleeding.
➤ Rupture of spleen.
➤ In pregnancy – Abortion, Stillbirth, Low birth weight and intrauterine death.
➤ Immunological disorders:
- Hyper-reactive malarial splenomegaly.
- Malarial nephrosis.
Recurrent Fever Pattern in Malaria:
-> Recrudescence.
-> Skeanned
Recrudescence
- It is the clinical manifestation which results from persistence of infection in blood,.
- In case of P. vivax and P. ovale – recrudescence may occur due to inadequate drug therapy.
- In case of P. falciparum and P. malariae – It occurs due to drug resistance when a person’s immunity is destroyed. It is recorded to occur upto 40 years after original attack in case of P. malariae
Relapse:
- It is the clinical manifestation results from persistence of blood infection and or persistence of exoerythrocyric forms in the liver in which erythrocytic schizogony commences again.
Treatment of Malaria:
A) Uncomplicated malaria:
| Day | Drug and dose | Tablet | Total dose |
| 1st | Chloroquine (150 mg) | 4 tab. single dose once after meal | 600 mg |
| 2nd | Chloroquine (150 mg) | 3 tab. single dose once after meal | 450 mg |
| 3rd | Chloroquine (150 mg) | 3 tab. single dose once after meal | 450 mg |
| 4th | Primaquine 15 mg | 3 tab. single dose | 45 mg |
B) Treatment of Chloroquine resistant malaria/Treatment failure malaria: In most areas of the world P. falciparum is now resistant to chloroquine
| Day | Drug and dose | Tablet | Total dose |
| 1st | Quinine 300 mg base | 2 tab. (8 hourly 3 times daily) | 600 mg |
| 2nd | Quinine 300 mg base | 2 tab. (8 hourly 3 times daily) | 600 mg |
| 3rd | Quinine 300 mg base | 2 tab. (8 hourly 3 times daily) | 600 mg |
| 4th | Quinine 300 mg base + Fansider | 2 tab. (8 hourly 3 times daily) + 3 tab. single dose 2 time daily | 600 mg |
On 8th day primaquine 15 mg single dose 3 tablet
C) Severe malaria/cerebral malaria:
a. Loading dose: Quinine dihydrochloride 20 mg/kg body weight by IV infusion
b. Maintenance dose: After 8 hours
- Quinine salt: 10 mg/kg body weight, over 4 hours by IV infusion
- Maintenance dose should be continued 8 hurly until the patient can swallow tab to complete the 7 day course
c. Fansidar single dose on the 3rd day
d. Primaquine single dose on the 4th day
Pathogenesis of Malaria:
➤ The parasite enters the mosquito’s stomach through the infected human blood obtained by biting or during blood meal.
➤ The parasite undergoes sexual conjugation.
➤ After 10 O to 14 days, a number of young parasites are released which work their way into the salivary gland of the mosquito.
➤ The organisms are carried in the saliva into the victim when the mosquito bites again.
➤ The female alone plays the role of a vector and definitive host in conveying the disease from man to man (sexual propagation).
➤ In humans, the organisms invade the RBC where they grow and undergo sexual schizogony
➤ Erythrocytic merozoites are produced leading to the rupture of RBC upon the release of the tiny organisms.
➤ Young merozoites invade a new batch of RBC, to start another schizonic cycle.
Prevention & Control of Malaria:
A. Measures to be applied by the individual:
- Prevention of man/Vector contact: Using repellants protection clothing bed-nets screening of houses.
- Destruction of adult mosquitoes: Use of domestic space spray
- Destruction of mosquito larvae: Peri-domestic sanitation intermittent during of water container
- Source reduction: Small scale drainage system
- Measures against malaria parasite: Chemoprophylaxis and chemotherapy
B. Measures to be applied by the community:
- Prevent of man/vector contact: Site selection and screening of houses
- Destruction of mosquito larvae: Using larvicides
- Source reduction: Prevention of manmade malaria environment sanitation water
management
C. Measures against malaria parasite: Presumptive treatment radical treatment mass drug administration.
Nursing Management of Malaria:
1. The patient must be closely monitored
- Intake and output should be closely monitored to prevent pulmonary edema,
- Daily monitoring of patient’s serum bilirubin, BUN creatinine, and parasitic count
2. If the patient exhibits respiratory and renal symptoms, determine the arterial blood gas and plasma electrolyte
3. During the febrile stage, tepid sponges, alcohol rubs, and ice cap on the head will help bring the temperature down.
4. Application of external heat and offering hot drinks during chilling stage is helpful.
5. Provide comfort and psychological support.
6. Encourage the patient to take plenty of fluids.
7. As the temperature falls and sweating begins, warm sponge bath maybe given.you
8. The bed and clothing should be kept dry
9. Watch for neurologic toxicity (from quinine infusion) like muscular twitching, delirium, confusion, convulsion, and coma.
10. Evaluate the degree of anemia,
11. Watch for any signs especially abnormal bleeding.
12. Consider severe malaria as medical emergency that requires close monitoring of vital signs
![]()