Prolong labour – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Prolong labour
Definition of prolong labour:
Prolonged labor is the inability of a woman to proceed with childbirth upon going into labor Prolonged labor typically lasts over 20 hours for first time mothers, and over 14 hours for women that have already had children.
Causes/risks factors of prolong labour:
- The baby is very big and cannot move through the birth canal.
- The baby is in an abnormal position. Normally, the baby is head-down facing your back.
- The birth canal is too small for the baby to move through.
- Contractions are very weak.
- low oxygen levels for the baby
- abnormal heart rhythm in the baby
- abnormal substances in the amniotic fluid
- uterine infection
Or
Risk factor/Causes of prolonged and arrested labor
Prolongation and arrest of labor are primarily due to conditions that cause mechanical impediments or inadequate contractions, both of which are discussed in this section.

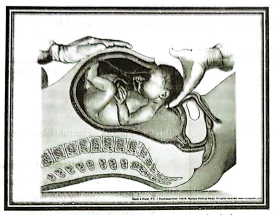
1. Fetal malpresentation: If the baby is not in the cephalic (vertex) position (in which the head is at the lower part of the abdomen) before birth, issues with labor progression can occur.
2. Cephalopelvic disproportion (CPD): CPD occurs when there is disproportion between the size of the fetus and the size of the maternal pelvis. This size mismatch can cause labor to slow or stop completely.
3. Problems with uterine contractions: Inadequate uterine activity occurs when contractions are either not sufficiently strong or not appropriately coordinated enough to dilate the cervix and push the baby out. Issues with uterine activity can arise due to a pregnancy with multiples, excessive use of painkillers or anesthesia, or a variety of other factors.
4. Maternal obesity: Higher maternal BMI (body mass index) is correlated with a longer first stage of labor, as well as a variety of other pregnancy complications.
Signs and symptoms of prolonged and arrested labor:
Signs and symptoms of prolonged and arrested labor
Labor that extends for more than 14-20 hours
❖ Maternal exhaustion and/or distress; dehydration may be present, and the mouth may be dry due to prolonged mouth breathing.
❖ Pain in the back and sides of the body, radiating out to the thighs due to prolonged strong pressure on the back
❖ Decrease in labor pains over time as the muscles become fatigued
❖ High pulse rate due to dehydration, exhaustion, and stress
❖ Dilation of the large intestines, which can be felt along both sides of the uterus as large, thick, air-filled structures
❖ The uterus is tender upon touch and does not relax fully between contractions
❖ Fetal distress may develop
❖ Abnormal contraction patterns which may include “coupling” (two contractions in rapid succession) or “tripling” (three contractions in rapid succession)
Diagnosing prolonged and arrested labor
❖ Whether signs and symptoms of the condition are present
❖ The duration of labor
❖ The frequency and strength of contractions
Whether labor is abnormal according to expert standards. A normal course of labor consists of the following stages:
1. Stage 1: There are uterine contractions leading to complete cervical dilation. This stage is divided into the latent and active phases. In the latent phase, irregular uterine contractions occur with slow and gradual cervical effacement and dilation. The active phase is demonstrated by an increased rate of cervical dilation and descent of the baby.
2. Stage 2: This is defined as complete dilation of the cervix to the delivery of the infant.
3. Stage 3: Stage 3 involves delivery of the placenta.
Complications of prolonged and arrested labor
When labor progresses slowly or stops completely, risks arise for both the mother and the baby. It is imperative that medical professionals act quickly to prevent serious long-term damage. The following are commonly associated with mismanaged prolonged or arrested labor (1):
Dangers to the fetus:
❖ Fetal distress due to oxygen deprivation
❖ Intracranial hemorrhage
❖ Increased use of forceps or vacuum extractors
❖ Sepsis
❖ Long-term risks of the baby developing permanent injuries, such as cerebral palsy, hypoxic-ischemic encephalopathy (HIE), and seizure disorders
Dangers to the mother:
❖ Intrauterine infections
❖ Trauma and injuries in the maternal birth passage (cervical tears, vaginal wall tears)
❖ Postpartum hemorrhage
❖ Postpartum infection
Oxytocin/Pitocin:
If a woman has a prolonged active phase of labor, physicians sometimes administer Pitocin; this is a synthetic hormone used to induce labor and strengthen uterine contractions. If used properly, Pitocin can speed up the labor process, effectively treating prolonged or arrested labor. Physicians may use Pitocin with the intent to avoid the need for C-section delivery;
however, it is essential that the risks and benefits of Pitocin use are heavily considered. If administered incorrectly or in high doses, Pitocin can cause tachysystole (excessive uterine contractions) which can jeopardize the baby’s oxygen supply and put both the mother and baby at risk.
It is important to note that Pitocin must be used with caution at any dose, and the individual clinical picture should be thoroughly considered before professionals proceed with Pitocin intervention.
Artificial rupture of membranes (amniotomy)
Artificial rupture of the membranes, or an amniotomy, is a procedure whereby the physician ruptures the woman’s membranes with a finger or special tool in order to accelerate labor. There is conflicting evidence regarding the effectiveness of amniotomy in speeding up the labor process. Used in combination with Pitocin, amniotomy may help to induce or augment labor.
However, it is important to note that there are risks associated with both Pitocin (as indicated above) and amniotomy. It has been suggested that amniotomy may treat prolonged or arrested labor because it may promote contraction.
However, there is no concrete evidence that amniotomy alone can induce labor, shorten labor, or prevent C-sections. The potential benefits of performing an amniotomy must be weighed against the risks of this procedure in order to make an informed decision.
Forceps and vacuum extractors
These are instruments that are used to assist in vaginal deliveries. If used properly, they can speed up the delivery of the baby. If used improperly, they can cause traumatic birth injuries, which can be permanent.
Injuries associated with improper use of these instruments include the following: hemorrhages (brain bleeds), seizures, Erb’s palsy, hypoxic-ischemic encephalopathy (HIE), and cerebral palsy. Because of these risks, forceps and vacuum extractors are not often used to manage prolonged or arrested labor.
C-section
A. C-section is performed when a vaginal delivery would put the baby or mother at risk. Some conditions that require the baby to be delivered immediately include fetal distress, uterine rupture, and cord prolapse. If labor is arrested in the first stage of labor, or if labor augmentation via Pitocin is unsuccessful, a C-section should be performed.
If a woman is at risk of having any type of abnormal labor, intensive clinical monitoring should be done. This includes recording the pulse, blood pressure, fetal heart sound (FHS), and dilation of the cervix. Fetal heart rate strips should be checked frequently. If in spite of the above procedures, labor fails to accelerate, or if fetal distress develops, an emergency C-section should be performed.
Pursuing legal help for a birth injury is one of the first steps you can take to secure a better life for your injured loved one. Obtaining compensation from a successful medical malpractice case will better allow your family to afford treatment, therapy, lifestyle adjustment, adaptive equipment, life care, and more.