Rupture Uterus – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Rupture Uterus
Uterine rupture:
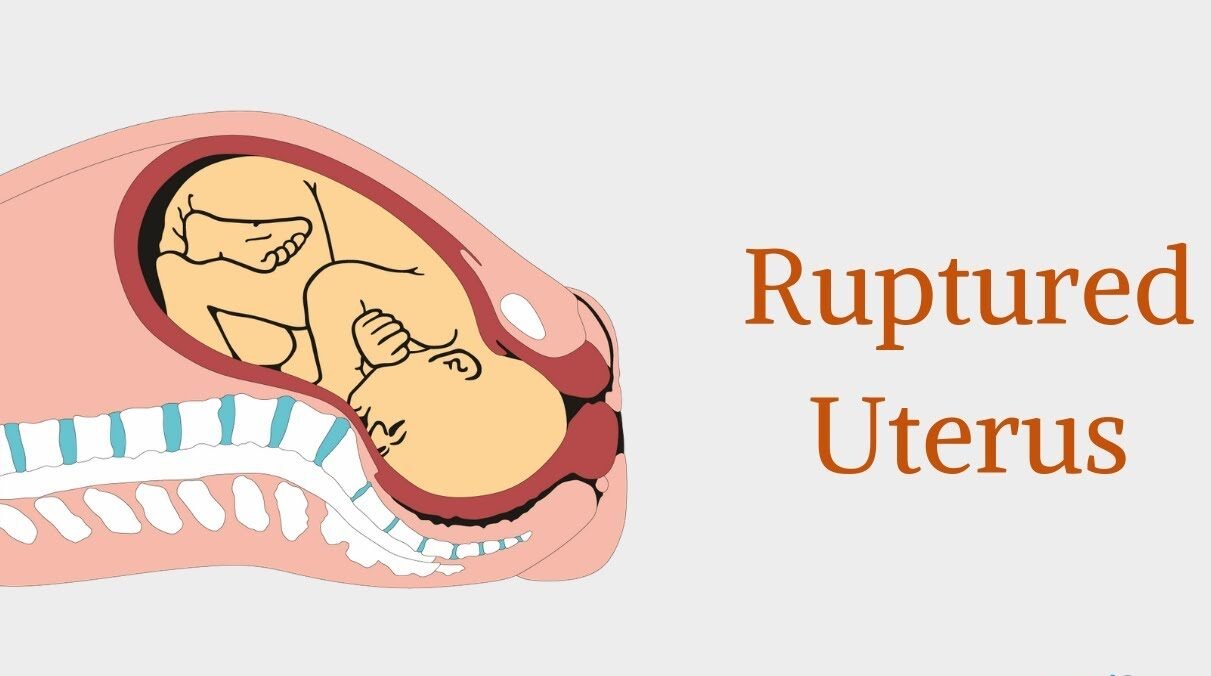
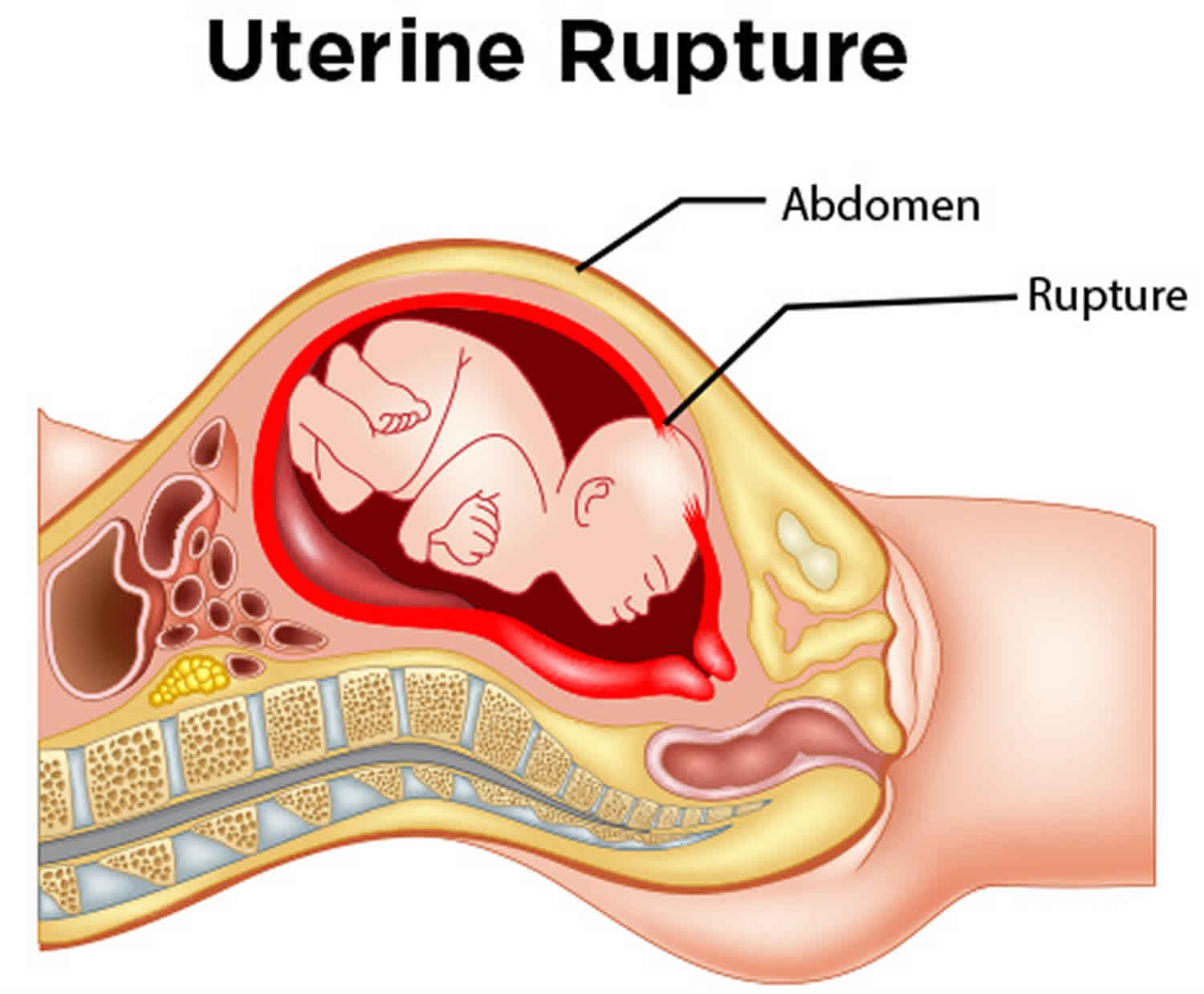
A uterine rupture is a tear in the wall of the uterus, most often at the site of a previous c-section incision. In a complete rupture, the tear goes through all layers of the uterine wall and the consequences can be dire for mother and baby.
Or
Uterine rupture is a rare childbirth complication that can occur during vaginal birth. It almost always occurs in women with uterine scars from previous caesarian sections or other uterine surgeries.

Risk factors of uterine rupture:
Pregnancy considerations include the following:
➤ Grand multiparity.
➤ Maternal age if the mother is above 35 years old.
➤ Placentation (accreta, percreta, increta, previa, abruption).
➤ Cornual (or angular) pregnancy.
➤ Uterine overdistension (multiple gestation, polyhydramnios).
➤ Dystocia (fetal macrosomia, contracted pelvis).
➤ Gestation longer than 40 weeks.
➤ Trophoblastic invasion of the myometrium (hydatidiform mole, choriocarcinoma).
Previous pregnancy and delivery history may include the following:
➤ Previous successful vaginal delivery.
➤ No previous vaginal delivery.
➤ Interdelivery interval.
Labor status is determined as follows:
➤ Not in labor.
➤ Spontaneous labor.
➤ Induced labor – with oxytocin, with prostaglandins.
➤ Augmentation of labor with oxytocin.
➤ Duration of labor.
➤ Obstructed labor.
Obstetric management considerations include the following:
➤ Instrumentation (forceps use).
➤ Intrauterine manipulation (external cephalic version, internal podalic version, breech extraction, shoulder dystocia, manual extraction of placenta).
➤ Fundal pressure.
Uterine trauma includes the following:
➤ Direct uterine trauma (eg, motor vehicle accident, fall).
➤ Violence (eg, gunshot wound, blunt blow to abdomen).
Causes of uterine rupture:
➤ Congenital uterine anomalies,
➤ Multiparity,
➤ Previous uterine myomectomy,
➤ Fetal macrosomia,
➤ Labor induction,
➤ Hydramnios,
➤ Uterineinstrumentation.
➤ Uterine trauma all increase the risk of uterine rupture.
➤Fetal distress.
➤ Sepsis – A uterine rupture increases the likelihood infection.
➤ Cerebral palsy.
➤ Developmental delay.
➤ Seizure disorders.
➤ Paralysis
➤ Mental retardation.
➤ Stillbirth
Signs of uterine rupture:
Several signs have been noticed prior to uterine rupture. However, all these signs do not necessarily happen with every uterine rupture. Uterine rupture is mostly accompanied with some
of the following signs:
➤ An abnormal heart rate of the baby (that is why the baby is monitored full time during VBAC- Vaginal Birth after Cesarean.
➤ Sudden sharp pain in the area of the previous scar.
➤ Baby’s head starts moving upward instead of going down the birth canal.
➤ Uterine atony, a condition in which the uterus loses its muscle tone.
➤ Abnormal abdominal pain.
➤ Chest pain,
➤ Hypovolemic shock caused by haemorrhage.
➤ Too much vaginal bleeding.
➤ Cessation of uterine contractions.
➤ Pain in the chest and rapid heart rate due to internal bleeding.
➤ The baby’s head appears to bulge under the pubic bone. This points out that the baby is outside the uterus.
➤ The contractions start to slow down and sudden pain appears during the contraction.
➤ Post-term pregnancy.
Signs of impending scar rupture during labour:
◆ Frequent, strong uterine contractions, occurring more than 5 times in every 10 minutes, and/or each contraction lasting 60-90 seconds or longer.
◆ Fetal heart rate above 160 beats/minute, or below 120 beats/minute, persisting for more than 10 minutes this is often the earliest sign of obstruction affecting the fetus.
◆ Bandl’s ring formation.
◆ Tenderness in the lower segment of the uterus.
◆ Possibly also vaginal bleeding.
Treatment of uterine rupture:
Once a uterine rupture is suspected, there are a number of ways in which it can be treated depending upon the severity of the case. These treatment methods are as follows:
1. Blood transfusion – Should excessive bleeding become an issue during a VBAC (Vaginal Birth After Cesarean), a blood transfusion may be a life-saving method for a mother who has suffered from a large loss of blood.
2. Hysterectomy – If a uterine rupture damages the uterus to the point where it cannot be saved, a hysterectomy may unfortunately be a woman’s only option.
3. IV antibiotics and fluids – A uterine rupture places you at greater risk of an infection. It may be necessary for you to receive life sustaining antibioties and IV fluids to compensate for the loss of blood.
4. Monitoring-patient will be monitored for a period of time after sustaining a post-rupture complication. During this time, patient will be urged to cat nutritious meals and drink plenty of fluids. Moreover, patient will likely be given iron supplements and advised to rest.
Nursing management of uterine rupture:
1. Before labor, review history for factors that places the women at risk for uterine rupture.
2. For women who have risk factors and all women have oxytocin induction/augmentation, monitoring fetal heart rate and uterine contraction, assess frequency, duration and intensity of uterine contraction.
3. Before labor, be sure that a type and screen has been done.
4. Report signs and symptoms of uterine rupture immediately to physician/midwife; call for help, do not leave the client.
5. Start or increase IV fluid.
6. Obtain blood immediately.
7. Oxygen should be administered.
8. If uterine rupture is suspected, deliver immediately by caesarian section and repair the uterus or perform hysterectomy.
9. Prepare the patient for immediate surgery.
10. Catheterization should be done.
11. Written informed consent should be taken.
12. Provide emotional support to the family.
Complications of uterine rupture: It is obstetric emergency because following complications may occur due to uterine rupture and that need emergency obstetrical care,
➤ Postoperative infection.
➤ Damage to ureter.
➤ Amniotic fluid embolus.
➤ Massive maternal haemorrhage and disseminated intravascular coagulation (DIC).
➤ Pituitary failures egna low
➤ Shock due to excessive haemorrhage.