Shaft of Humarus fracture- An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.
Shaft of Humarus fracture
Causes of shaft of humerus fracture:
1) Usually result from a direct blow.
2) Occasionally due to a fall, or twisting motion, on an outstretched hand.
3) Rarely have been reported after strenuous exercise caused by violent muscle contraction.
4) Fracture pattern tends to relate to the muscular attachments.
3. Bruising and angulation are often present.
4. The arm may be shortened and rotated depending on the fracture displacement.
5. Fracture crepitus is common with complete fractures.
6. Suspect radial nerve damage if there is a wrist-drop or sensory impairment in the dorsal aspect of the 1st web space.
7. Swelling.
8. Deformity.
9. On palpation:
a. Tenderness.
b. Abnormal mobility and
c. Bony crepitatus
d. Examine the neuro-vascular supply of the limb.

[Ref-Dr. M.A.H.M. Jafar’s “Fracture and Dislocations” 2nd edition]
Radiological features of shaft of humerus fracture:
1. AP (anterior and posterior) and lateral are essential as a displaced fracture can be underestimated on one view.
2. Fractures tend to be mid-shaft and transverse.
3. Incomplete fractures can be subtle. Look for cortical break at the site of maximum tenderness.
4. If fracture occurs above pectoralis major insertion, the proximal fragment abducts. If between pectoralis major and deltoid insertions, the proximal fragment will adduct. If distal to deltoid insertion, the proximal fragment will abduct.
Manage a case of shaft of humerus fracture:
A) Conservative methods
1) Analgesia and immobilised
2) Closed single fractures are best treated by a plaster U slab or functional cast brace
3) A hanging cast is recommended for grossly displaced or comminuted Fractures The cast should be lightweight as a heavy cast will increase the risk of excess distraction and non-union. Reassess neurology post-cast application.
4) Follow-up in the fracture clinic.
5) If severely displaced/comminuted, multiple, open or associated with neurology, the patient should be referred to the orthopaedic team immediately.
B) Operative methods:
1) Compression plate and screw.
2) Interlocking intramedullary nail
3) External fixator.
Indications of operative treatment :
1. Failed conservative treatment.
2. Multiple fractures and unstable fractures.
3. Multisystem injuries.
4. Radial nerve palsy after closed reduction.
5. Pathological fractures.
6. Compound fractures with vascular injuries.
7. Segmental fractures.
8. Intra-articular extension into shoulder and elbow joints. يسا
9. Bilateral humeral fractures.
10. Brachial plexus injuries.
11. Ipsilateral shoulder or forearm fractures.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-142]
Complications of fracture shaft humerus :
A) Early complication:
1) Vascular injury-Direct repairing or grafting is needed immediately
2) Nerve injury- radial nerve palsy (Wrist drop).
B) Late complications:
1) Delayed union.
2) Non-union.
3) Mal-union.
4) Stiffness of shoulder joint.
5) Osteoporosis.
6) Myositis ossifications.
[Ref-Apley’s “System of Orthopaedics and Fractures” 9th edition page-735]
Supracondylar Fracture of Humerus
Supracondylar fracture:
Fracture through the supracondylar region of the humerus is known as Supracondylar fracture of humerus.
[Ref-Dr. Jahir, “Surgery 1st Paper” 4th Edition,Page-549]
Supracondylar fracture of humerus:
1) Extension (Common)
2) Flexion type.
Supracondylar fracture of humerus :
Anatimical peculiarity: Due to thin fat lower end and presence of olecranon (Posteriorly) & Coracoid fossa
(Anteriorly).
Frequent fall mon the elbow :
- Fall in out stretched hand slightly flexed elbow during playing.
- Fall from height.
- RTA.
[Ref-Dr. Jahir, “Surgery I” Paper” 4th Edition, Page-5491]
Clinical features of Supracondylar fracture of humerus:
A) Patient profile: Commonest fracture of children between 5-10years.
B) Symptoms:
H/O fall on elbow(Fall in semi flexed elbow on outstretched hand) Pain on the elbow joint. Swelling around the elbow joint.
Deformities at the back of the elbows. Restricted movement at the back of the elbow,
C) Signs:
Swelling around the elbow joint.
Very much tender-child may not allow to touch.
Crepitus may be felt.
Movement of the elbow is very much painful and restricted.
[Ref-Dr. Jahir, “Surgery It Paper” 4th Edition, Page-549]
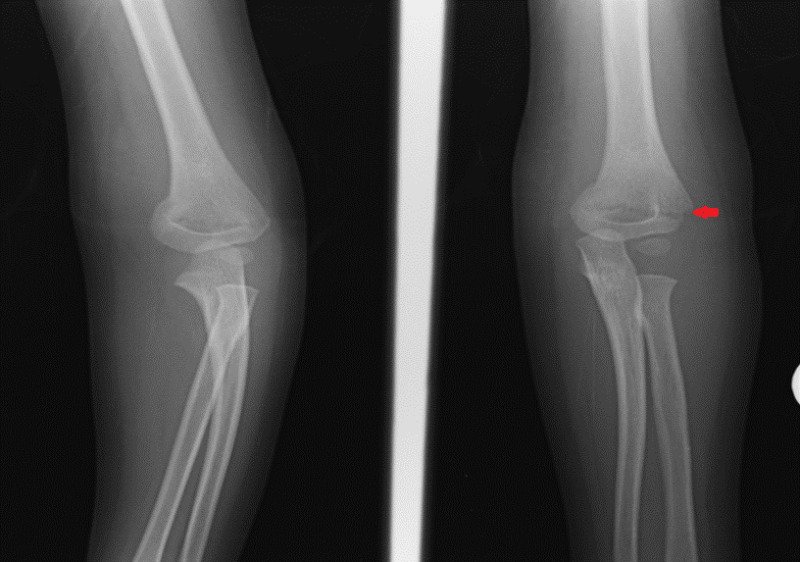
Radiological feature of Supracondylar fracture of humerus:
1) Obtain an AP and lateral view of the elbow.
2) A spectrum of abnormalities can be seen from mild cortical irregularity to complete displacement of the distal humeral fragment with loss of fracture continuity.
3) Often only a subtle fracture line will be seen.
4) Look for the presence of a posterior fat pad, prominent anterior fat pad or disruption of the anterior humeral line.
Management of Supracondvlar fracture of humerus :
A) Undisplaced fracture: Immobilization by long arm back slab for 3 weeks.
B) Displaced fracture: Reduction by traction and counter traction under G/A followed by long arm back slab with elbow <90 degree for 3 weeks.
[Ref-Dr. Jahir, “Surgery 1″ Paper” 4th Edition, Page-549]

Complication of Supracondylar fracture of humerus :
A) Immediate complication:
1. Vascular injury:
a. Occlusion of brachial artery
b. Volkmann ischaemia
c. Grangrene.
2. Neuroligical injury:
- Radial nerve injury
- Median nerve injury
B) Late complication:
1) Volkmann ischarmia contracture.
2) Malunion
3) Cubitus varus
4) Cubitus valgus.
5)Non-union.
6) Myositis ossification.
7) Tardy nerve palsy.
8) Stiffness of elbow.