Thiazide Diuretics – This book covers the entire syllabus of “Pharmacology” prescribed by BNMC- for diploma in nursing science & midwifery students. We tried to accommodate the latest information and topics. This book is an examination setup according to the teachers’ lectures and examination questions.
At the end of the book, previous questions are given. We hope in touch with the book students’ knowledge will be upgraded and flourish. The unique way of presentation may make your reading of the book a pleasurable experience.
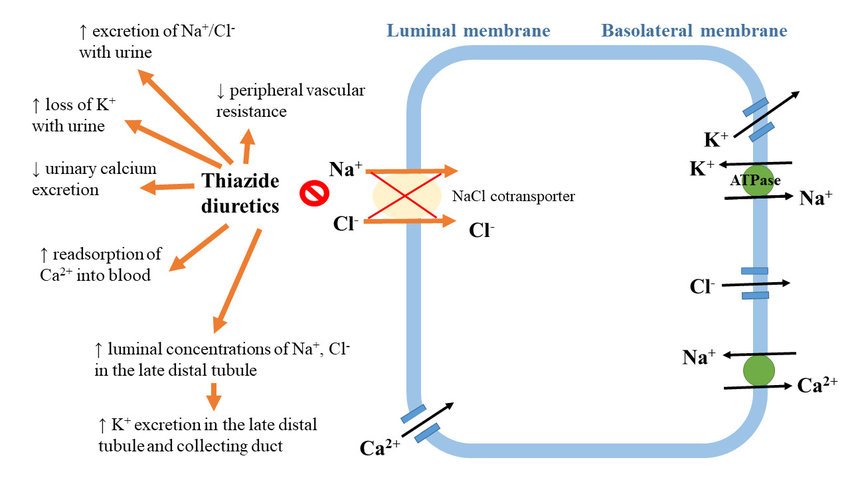
Thiazide Diuretics
Mechanism of Action
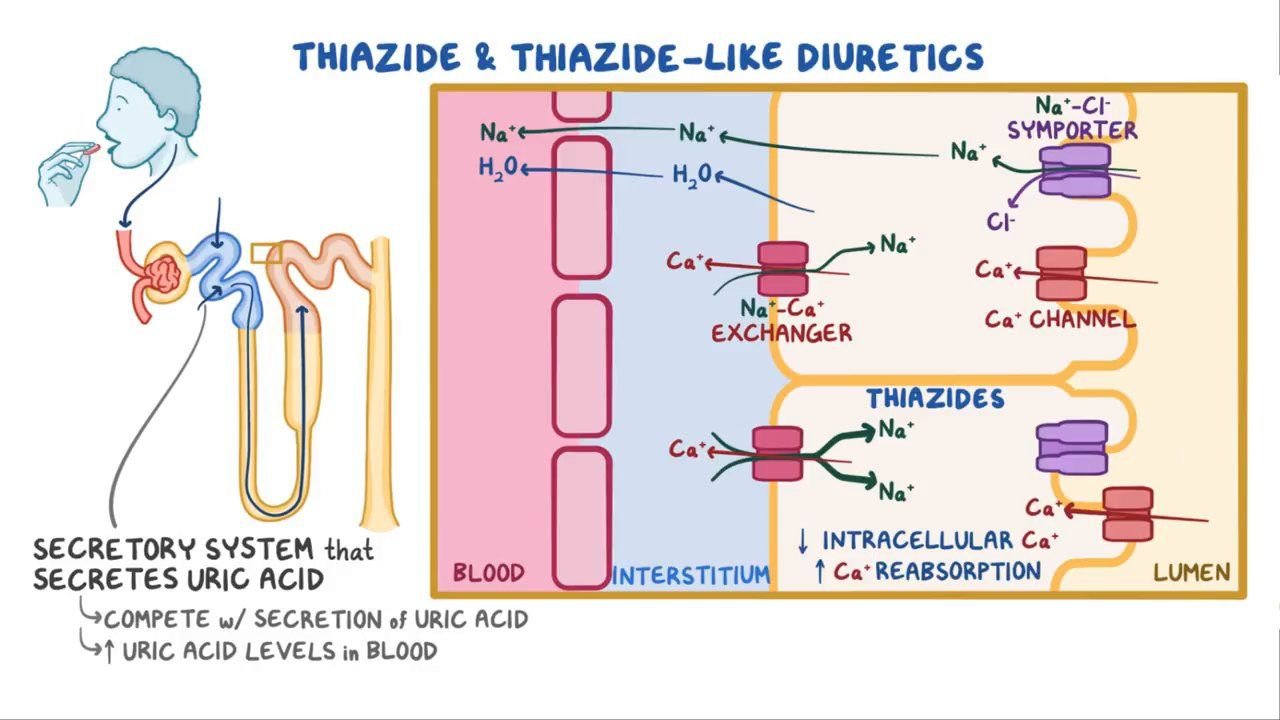
Inhibit Na+ -CI symporter in the distal convoluted tubules thereby reducing Na+ reabsorption and reducing water reabsorption.
Indications
- Hypertension
- Oedema in heart failure
Cautions and Contra-Indications
- Electrolyte disturbances (including refractory hypokalaemia, hyponatraemia, hypercalcaemia and symptomatic hyperuricaemia).
- Addison’s disease
- Avoid in breastfeeding mothers due to suppression of lactation
Side-Effects
- Postural hypotension
- Hyponatraemia
- Hypokalaemia
- Hyperuricaemia (e.g. gout)
- Hypercalcaemia
- Hyperglycaemia
- Male sexual dysfunction
- Suppression of lactation
- Raised LDL cholesterol
Metabolism and Half-Life:
Metabolised in the liver t½ is 3-4 h.
Monitoring:
Monitor plasma electrolytes for adverse effects as above.
Drug Interactions:
- Enhanced hypotensive effect with other antihypertensives
- Increased risk of nephrotoxicity with NSAIDs
- Reduced hypoglycaemic effect of oral antidiabetic agents.
Important Points
Thiazides are less effective than loop diuretics because 90%of Nat has been reabsorbed by the time the filtrate reaches the distal convoluted tubule Hypokalaemia results from increased activity of Na+/K+ ATPase in collecting ducts. This is caused by increased Na+ in filtrate and an aldosterone-mediated effect (diuretic-induced hypovolaemia causes activation of the renin-angiotensin-aldosterone system)
Carbonic Anhydrase Inhibitors
Carbonic anhydrase (CAse) is an enzyme which catalyses the reversible reaction H2O + CO2 H2CO3. Carbonic acid spontaneously ionizes H₂CO).
Acetazolamide:
It is a sulfonamide derivative which noncompetitively but reversibly inhibits CAse (type II) in PT cells resulting in slowing of hydration of CO2 decreased availability of H+ to exchange with luminal Na+ through the Na+-H+ antiporter.
Pharmacokinetics
Acetazolamide is well absorbed orally and excreted unchanged in urine. Action of a single dose lasts 8-12 hours.
Uses:
Because of self-limiting action, production of acidosis and hypokalaemia, acetazolamide is not used as diuretic. Its current clinical uses are:
- Glaucoma: as adjuvant to other ocular hypotensives.
- To alkalinise urine: for urinary tract infection or to promote excretion of certain acidic drugs.
- Epilepsy: as adjuvant in absence seizures when primary drugs are not fully effective
- Periodic paralysis.
Adverse effects are frequent
- Acidosis
- Hypokalaemia
- Drowsiness
- Paresthesias
- Fatigue
- Abdominal discomfort
- Hypersensitivity reactions-fever, rashes
- Bone marrow depression is rare but serious
Potassium Sparing Diuretics
Aldosterone antagonists and renal epithelial Na+ channel inhibitors indirectly conserve K+ while inducing mild natriuresis, and are called ‘potassium sparing diuretics
Spironolactone
It is a steroid, chemically related to the mineralocorticoid aldosterone. Aldosterone penetrates the late DT and CD cells and acts by combining with an intracellular mineralocorticoid receptor (MR) induces the formation of ‘aldosterone-induced proteins’ (AIPs).
Pharmacokinetics
The oral bioavailability of spironolactone from microfine powder tablet is 75%. It is highly bound to plasma proteins and completely metabolized in liver; converted to active metabolites, the most important of which is Canrenone that is responsible for 1/2-2/3 of its action in vivo. The t½ of spironolactone is 1-2 hours, while that canrenone is -18 hours. Some enterohepatic circulation occurs.
Use
Spironolactone is a weak diuretic in its own right and is used only in combination with other more efficacious diuretics.
- To counteract K+ loss due to thiazide and loop diuretics.
- Edema:
- Hypertension
- CHF
Interactions
- Given together with K+ supplements dangerous hyperkalaemia can occur.
- Aspirin blocks spironolactone action by inhibiting tubular secretion of its active metabolite canrenone.
- More pronounced hyperkalaemia can occur in patients receiving ACE inhibitors/ARBs.
- Spironolactone increases plasma digoxin concentration.
Adverse effects
The side effects are drowsiness, ataxia, mental confusion, epigastric distress and loose motions.