Tibial fracture – An orthopedic nurse is a nurse who specializes in treating patients with bone, limb, or musculoskeletal disorders. Nonetheless, because orthopedics and trauma typically follow one another, head injuries and infected wounds are frequently treated by orthopedic nurses.
Ensuring that patients receive the proper pre-and post-operative care following surgery is the responsibility of an orthopedic nurse. They play a critical role in the effort to return patients to baseline before admission. Early detection of complications following surgery, including sepsis, compartment syndrome, and site infections, falls under the purview of orthopedic nurses.

Tibial fracture | CHAPTER 5 | Orthopedic Nursing
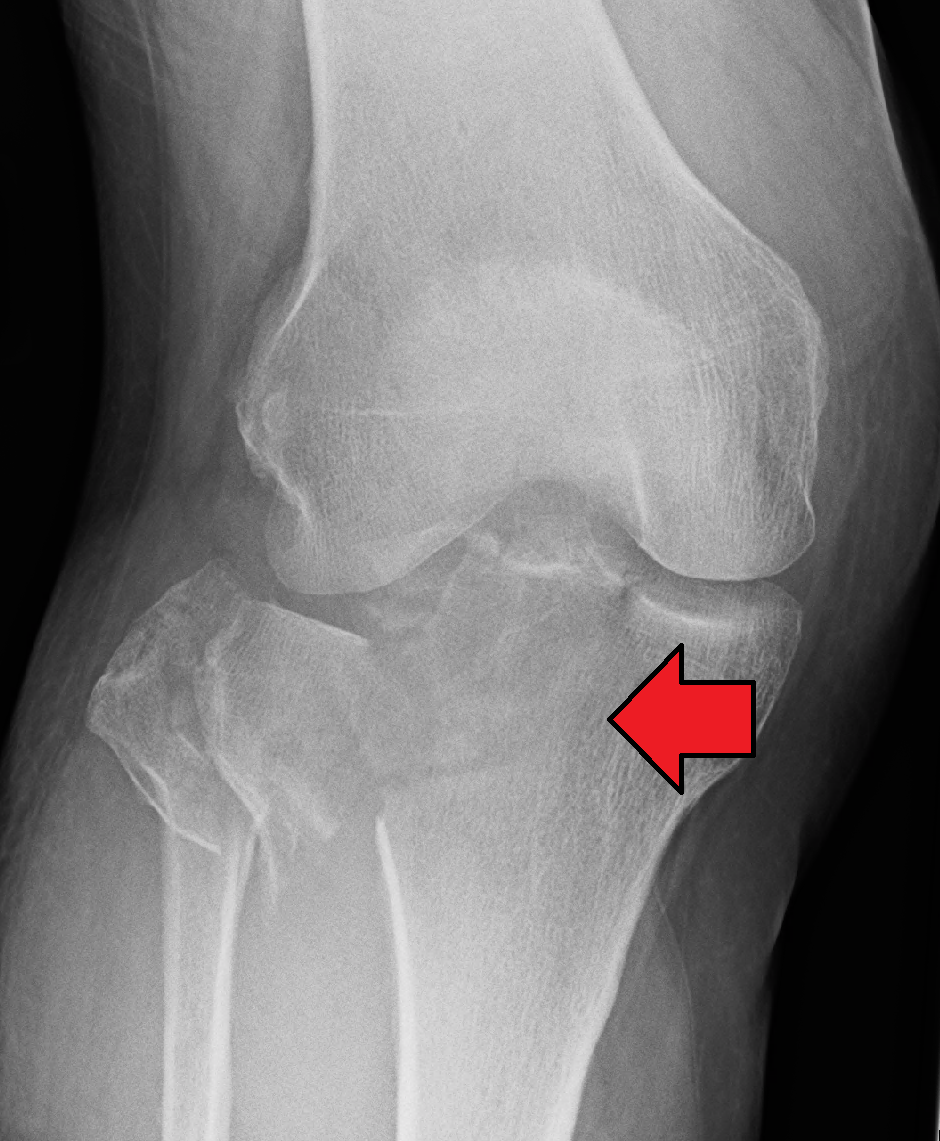
Clinical features of tibil fracture:
1) Pain, swelling and deformity are common. Deformity or angulation may be seen. The foot may be abnormally rotated.
2) Although vascular injuries are rare, it is important to assess distal pulses.
3) ‘Foot drop’ occurs with common peroneal nerve damage. Assess sensation in the first dorsal web space of the foot (deep peroneal nerve).
4) Ligamentous knee disruption is not uncommon and may be missed.
Treatment of tibial fracture:
4) Undisplaced fracture: Immobilization in long leg full plaster (LLFP) for 6 weeks followed by cast brace.
5) Displaced fracture: Reduction under G/A,external immobilization in plaster cast.nad sitt on le
6) Unstable fracture: Skeletal traction, external fixator „External fixation with plate and screw.
[Ref-Dr. Jahir, “Surgery I” Paper” 4th Edition, Page-560]
Follow us on Google news
Indications of operative treatment in tibial fracture :
1) Tibial fracture with vascular or neural injuries.
2) Segmental fractures.
3) Inadequate reduction.
4) Associated knee problems.
5) Associated tibial plafond fracture.
Advantages:
1) Deformity form of treatment.
2) No loss of position or shortening.
3) No postfracture deformity.
4) Joint movements obtained early.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-269-270]
Complications of tibial fracture:
1) Delayed union.
2) Nonunion.
3) Infected nonunion.
4) Mai-union.
5) Shortening.
6) Infection.
7) Compartmental syndromes.
8) Joint stiffness
9) Refracture.
10) Fat embolism
11) Claw toes due to tethering of long extensors over callus.
[Ref-John Ebnezar’s “Textbook of Orthopedics” 4th edition page-272]