Instrumental deliveries – This course is designed to understand the care of pregnant women and newborn: antenatal, intra-natal and postnatal; breast feeding, family planning, newborn care and ethical issues, The aim of the course is to acquire knowledge and develop competencies regarding midwifery, complicated labour and newborn care including family planning.
Vacuum extraction/ventouse delivery
Ventouse delivery:
Ventouse is an instrumental device designed to assist delivery by creating a vacuum between it & the fetal scalp.
The pulling force is dragging the cranium while in forceps the pulling force directly transmitted to the base of the skull.
[Ref-D. C. Dutta’s Obs/9/538]
Pre-requisite of vacuum extraction:
1. Presentation: Presentation must be vertex & preferably well flexed.
2. No evidence of cephalo-pelvic disproportion.
3. There should not be slightest bony resistance below the head.
4. Cervix should be at least 6cm dilated (preferably only cervical rim may be Left behind).
[Ref-D. C. Dutta’s Obs/9/533]
Indications of Ventose delivery:
- As an alternative to forceps operation.
- As an alternative to rotational forceps as in occipito transverse or posterior position.
- Delay in descent of the head in case of the 2nd baby of twins.
- Delay in the first stage of the labour (uterine inertia).
Contra-indication of ventouse delivery:
- Any presentation other than vertex (face, brow breech);
- Preterm fetus (< 34 weeks): Chance of scalp avulsion or subaponeurotic haemorrhage.
- Suspected fetal coagulation disorder.
- Suspected fetal macrosomia.
[Ref-D. C. Dutta’s Ohs/9/539]
Procedure of Ventrose delivery:
- Lithotomy position.
- Antiseptic measures for the vagina, vulva and perineum.
- Vaginal examination to check pelvic capacity, cervical dilatation, presentation, position, station and degree of flexion of the head and that the membranes are ruptured.
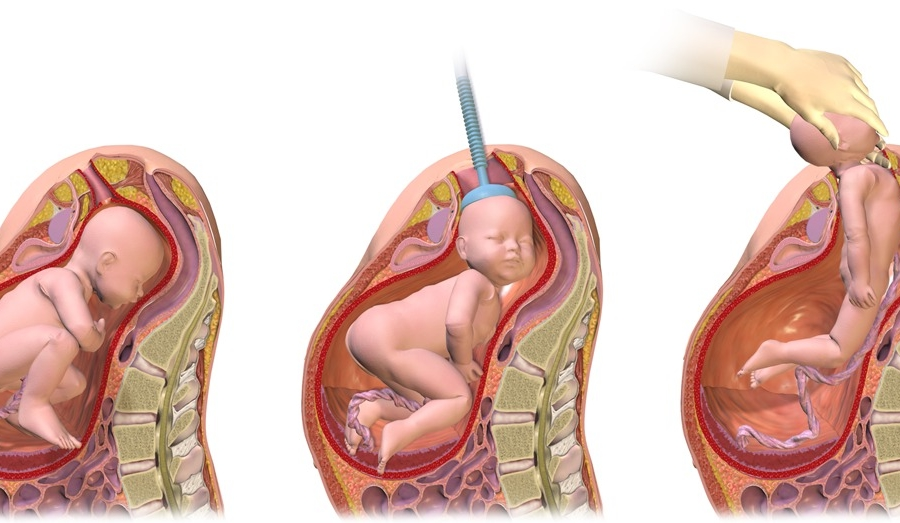
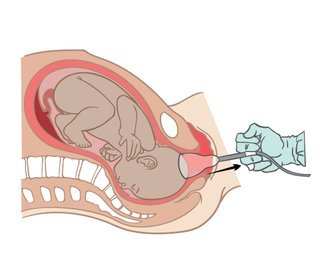
- Application of the cup: The largest cup that can easily passed is introduced sideways into the vagina by pressing it backwards against the perineum. It is then applied as near as possible to the posterior fontanelle over the mid sagittal line with its edge 3 cm from the anterior fontanelle. This position will promote flexion of the head and brings the smallest diameters of the foetal skull into the maternal passages. Be sure that there is no cervical or vaginal tissues nor the umbilical cord or a limb in complex presentation is included in the cup.
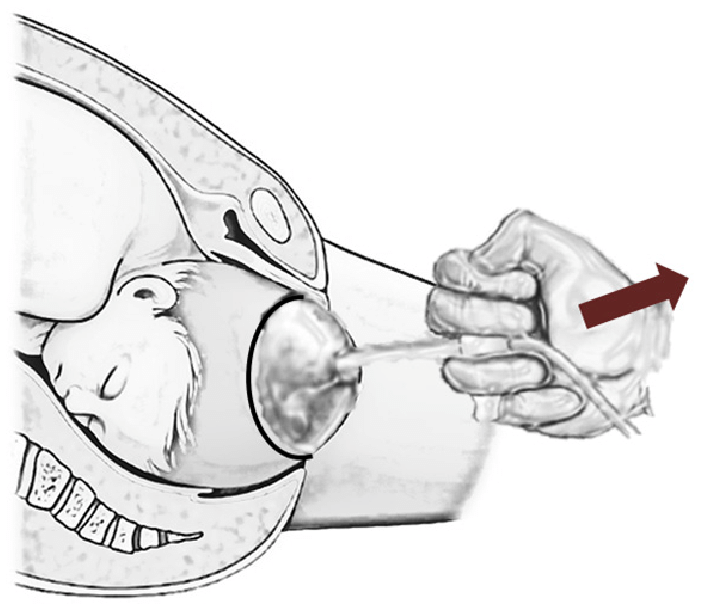
Creating the negative pressure: holding the cup in place, the negative pressure is
gradually increased by 0.2 kg/cm² every 1 minute until 0.8 kg/cm² is attained. This creates an artificial caput within the cup. - Traction: on the handle is made perpendicular to the cup and intermittently during uterine contractions, the direction of pull is changing as the head descends through the birth canal
- Release of the cup: when the head is delivered the vacuum is reduced as slowly as it was created using the screw as this diminishes the risk of scalp damage.
Bird’s safety rules for vacuum extraction:
◆ The head must be completely or partially delivered with no more than 3 pulls.
◆ The head is at least begin to move with the first pull.
◆ The cup must not be applied more than twice.
◆ Application of the cup must not exceed 20 minutes.
Complications of ventouse delivery:
Maternal complications:
The injuries are uncommon but may be due to inclusion of the soft tissues such as the cervix or vaginal wall inside the cup.
1. Vaginal and cervical lacerations.
2. Annular detachment of the cervix, cervical incompetence and may be future prolapse if used with incompletely dilated cervix.
Fetal complications:
1. Superficial scalp abrasion.
2. Sloughing of the scalp.
3. Cephalhaematoma due to rupture of emissary veins beneath the periosteum
4. Sub-aponeurotic/subgalealhaemorrhage (not limited by suture line as it is not subperiosteal).
5. Intra-cranial haemorrhage (no long term effect).
6. Retinal haemorrhage.
[Ref-D. C. Dutta’s Obs/9/5411]
Advantages of ventouse delivery over forceps delivery:
- It can be used in unrotated&malrotatedoccipito-posterior position of the head.
- It can be applied even through incompletely dilated cervix.
- Lesser traction force is needed.
- It is not a space occupying device like the forceps blades.
- It can be used safely even when the head remains at a high level & exact position is unsure.
- It is comfortable & injuries to the mother are less.
- Fetal complications are less.
- Required less technical skill (suitable for trained midwives).
Advantages of forceps over ventouse delivery:-
- In suspected pelvic contraction, where moderate traction is required, ventouse will be ineffective.
- Forceps operation can quickly expedite the delivery in case of fetal distress where ventouse will be unsuitable as it takes longer time.
- It is safer in premature baby.
- It can be employed in anterior face or in after-coming head of breech.
- Chance of cephalhaematoma is less compared to ventouse.
- Simplicity of the instrument, less costly & handy.
- Less failure rate compared to ventouse.
[Ref-D. C. Dutta’s Obs/8/660-663]